In a landmark shift for the treatment of cardiovascular and neurological conditions, the National Institute for Health and Care Excellence (NICE) has issued new guidance that promises to fundamentally alter how clinicians prescribe antiplatelet therapy following a stroke. By integrating genomic testing into standard clinical pathways, the NHS is set to move away from a "one-size-fits-all" approach to medicine, instead embracing a model of personalized care that identifies which patients may be at risk of harm from standard treatments.
The guidance centers on the use of genetic testing to determine a patient’s compatibility with clopidogrel, a cornerstone medication used to prevent secondary ischaemic strokes and transient ischaemic attacks (TIAs). By identifying specific genetic variants before a prescription is issued, clinicians can now pivot to alternative treatments for patients whose bodies are unable to properly metabolize the drug, potentially saving thousands of lives and reducing the economic burden on the healthcare system.
Main Facts: The Intersection of Genetics and Stroke Prevention
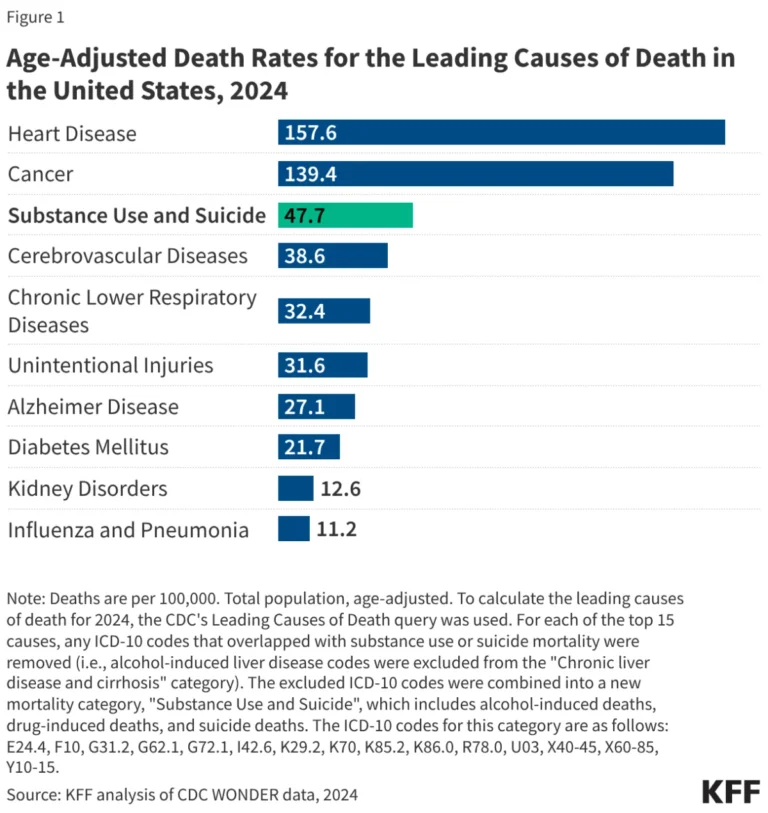
Each year in the United Kingdom, approximately 100,000 people suffer a stroke. It remains the fourth leading cause of death and the primary driver of long-term disability nationwide. Strokes are broadly categorized into two types: haemorrhagic, caused by a burst blood vessel, and ischaemic, where blood flow to the brain is obstructed by a clot. For the latter, clopidogrel is the standard-of-care, working as an antiplatelet agent that reduces the "stickiness" of platelets to prevent further clotting.
However, the efficacy of clopidogrel is not universal. Clinical research has identified that approximately 32% of the UK population carries a variant in the CYP2C19 gene. This gene is responsible for producing the enzyme that converts clopidogrel from an inactive "prodrug" into its active, therapeutic form. Individuals with this specific genetic variant process the drug inefficiently, rendering it significantly less effective.
Most alarmingly, evidence suggests that patients with the CYP2C19 variant who are treated with clopidogrel face a 46% higher risk of experiencing a recurrent stroke compared to those with a functional genotype. The new NICE guidance mandates that clinicians utilize genomic testing—either through traditional laboratory methods or rapid point-of-care testing (POCT)—to screen for this variant, ensuring that patients receive the most effective therapy for their specific genetic profile.
Chronology: From Research Validation to National Implementation
The journey toward implementing pharmacogenomics in stroke care has been a multi-year effort involving academic, clinical, and regulatory stakeholders.
- June 2023: Early reports began circulating regarding the viability of point-of-care testing (POCT) as a solution to the traditional diagnostic bottlenecks. Researchers highlighted the urgent need to bridge the gap between genomic discovery and bedside application.
- April 2024: NICE opened a period of public and professional consultation, seeking expert commentary on the proposed guidelines for post-stroke and mini-stroke prescribing. This period was critical for aligning the views of neurologists, geneticists, and health economists.
- Late 2024: Following the review of evidence, NICE officially published its guidance (DG59), formally recommending the use of CYP2C19 testing.
- The Pilot Phase: In conjunction with NHS England, a national pilot program is currently being structured. This phase is designed to stress-test the deployment of these genomic diagnostics within hospital environments, ensuring that the technology is robust enough to handle the volume of patients arriving in stroke units daily.
Supporting Data: The Scale of the Challenge and Opportunity
The clinical case for pharmacogenomics in this context is built on hard data. The 32% prevalence of the CYP2C19 variant means that roughly one in three stroke patients may currently be receiving sub-optimal therapy. When extrapolated across the 100,000 annual stroke cases, this represents a significant segment of the patient population whose secondary prevention strategies are effectively compromised by their own biology.
Dr. John McDermott, an NIHR doctoral research fellow and clinical genetics specialty registrar at the University of Manchester, underscores the magnitude of this change. "Over 100,000 patients a year are affected by stroke, so this will fundamentally change the landscape of pharmacogenomics in this country," he notes.
The economic implications are equally profound. Adverse drug reactions—where medications are ineffective or cause unintended harm—are a massive drain on NHS resources. Estimates suggest that patients suffering from such reactions occupy approximately 8,000 hospital beds at any given time. With the costs of these complications measured in the billions of pounds, the implementation of a rapid, bedside genetic test acts as a proactive cost-containment strategy. By ensuring the correct medication is administered at the start of the treatment plan, the NHS can reduce the incidence of preventable readmissions, shorten recovery times, and optimize the use of critical care resources.
Official Responses and Strategic Development
The development of the rapid, non-invasive POCT has been a collaborative success between clinical researchers and private sector innovators. The Manchester-based company Genedrive has been instrumental in the validation of the testing hardware. The device, which uses a simple cheek swab, can deliver results within an hour, fitting seamlessly into the fast-paced environment of an acute stroke unit.
NICE has adopted a pragmatic approach to the rollout, acknowledging the current limitations of laboratory-based infrastructure. While laboratory testing remains the gold standard for clinical precision, the organization is fully supportive of the POCT model as a bridge for the interim period. This dual-track strategy ensures that hospitals in varying geographical locations and with different resource levels can begin implementing the guidance immediately.
"We’ve developed a test where you take a cheek swab and put it into a machine, and it will produce a result to help guide anti-platelet therapy within an hour," says Dr. McDermott. "It’s a really exciting development that we’ve just finished validating, and the results are extremely impressive."
Implications: A New Era for Pharmacogenomics
The move toward routine genomic testing in stroke care is a harbinger of a broader transformation in the National Health Service. By proving that rapid genetic screening is both feasible and cost-effective for stroke, the NHS creates a template for similar interventions in oncology, cardiology, and psychiatry.
1. Patient Safety and Quality of Life
The primary implication is the immediate improvement in patient outcomes. For a patient who has already suffered a life-altering event like a stroke, the anxiety of recurrence is significant. Knowing that their medication has been "genetically tailored" provides a psychological and physiological safety net that standard prescribing cannot offer.
2. Operational Efficiency
The transition to a bedside testing model removes the "waiting period" associated with traditional laboratory diagnostics. In acute medicine, time is brain. By obtaining genetic results within the hour, clinicians can make informed decisions before the patient is even discharged, eliminating the need for subsequent adjustments to medication or, worse, the re-admission of a patient who suffered a second stroke.
3. Systemic Sustainability
While the initial implementation of testing equipment requires investment, the long-term savings are compelling. A system that prevents unnecessary hospital stays and reduces the need for expensive secondary treatments is a more sustainable system. The success of this pilot will likely serve as the business case for future investments in point-of-care genomics across the UK.
4. A Blueprint for the Future
The integration of this guidance signals that the NHS is moving away from a reactive healthcare model toward a proactive, preventative, and personalized one. The challenge now lies in the scale-up—ensuring that every stroke unit in the country has the equipment and training necessary to utilize these diagnostics effectively.
As the NHS continues to monitor the impact of this guidance, the medical community remains optimistic. The transition from generalized prescribing to precision medicine is no longer a theoretical goal; it is an active clinical reality. For the thousands of patients who will receive their care under these new protocols, the benefits—in the form of improved health and reduced risk—will be tangible and lasting.
Disclaimer: This article is for informational and educational purposes only and does not constitute professional medical advice. Always seek the guidance of a physician or other qualified health provider with any questions you may have regarding a medical condition or treatment.