Introduction: A New Paradigm for Global Health
The announcement of a severe Ebola outbreak in the Democratic Republic of the Congo (DRC) has sent shockwaves through the international health community. Escalating rapidly across the northeastern provinces and spilling over into neighboring Uganda, this health crisis is unfolding at a precarious moment in global governance. As international cooperation faces unprecedented strain, this outbreak serves as the first major “stress test” for the current global health architecture, particularly following significant policy shifts within the United States administration regarding foreign assistance and global health funding.
The convergence of a highly volatile, infectious pathogen with a complex, evolving fiscal landscape creates a scenario that experts fear may overwhelm existing response mechanisms. With regional stability at stake, the eyes of the world are fixed on how the international community—and the U.S. in particular—navigates this emergency under a new, less predictable, and more restrictive diplomatic framework.
Chronology of the Escalation
The timeline of this outbreak highlights the alarming speed at which the virus has traveled across borders.
- May 15, 2026: Initial reports emerged of a significant Ebola outbreak concentrated in the northeastern regions of the DRC. Preliminary data suggested a rapid spread, characterized by high transmission rates in both rural and semi-urban communities.
- May 17, 2026: Recognizing the gravity of the situation, the Director-General of the World Health Organization (WHO) formally declared the event a "Public Health Emergency of International Concern" (PHEIC). This designation was driven by two factors: the sheer volume of suspected cases and the verified transmission of the virus into Uganda.
- May 20, 2026: Within five days of the initial announcement, the scale of the crisis became clear. Epidemiological data reported nearly 600 suspected cases and more than 139 suspected deaths. The rapid climb in these figures indicates that the virus is outpacing initial containment efforts, raising concerns about the potential for further regional contagion.
The Nature of the Threat: Why This Outbreak is Different
While the global health community has gained significant experience responding to Ebola—notably during the West African epidemic of 2014-2015 and the cyclical outbreaks in the DRC between 2018 and 2020—this current crisis presents a distinct set of obstacles.
1. Structural and Logistic Hurdles
The geography of the northeastern DRC is notoriously difficult for rapid response teams. Poor infrastructure, including limited road networks and restricted access to remote areas, complicates the distribution of medical supplies and vaccines. Furthermore, the region is marked by ongoing socio-political instability, which inhibits the ability of healthcare workers to conduct contact tracing safely.
2. The Policy Landscape
This outbreak is the first of its scale to occur following the recent policy reorientations of the U.S. administration. Previous Ebola responses were largely underpinned by robust, predictable U.S. funding and direct diplomatic leadership. Current policy shifts toward "America First" frameworks in foreign aid have created uncertainty regarding the consistency of financial and logistical support. The transition from established, long-term funding models to more ad-hoc, project-based assistance has left many international partners questioning the depth of the U.S. commitment.
Supporting Data and the Regional Impact
Data visualization from current health clusters indicates that the current strain is exhibiting a higher-than-average infection rate compared to recent historical benchmarks. The spread into Uganda is particularly alarming; it marks the first time in recent years that a cross-border movement of this specific strain has occurred so quickly.
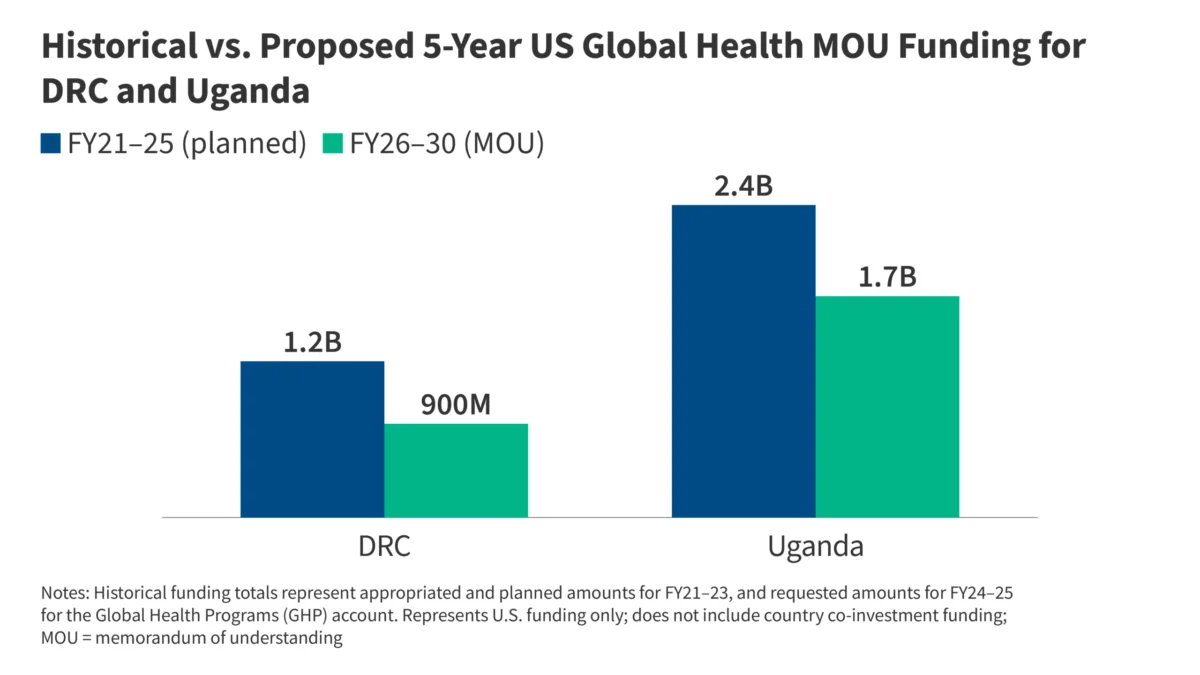
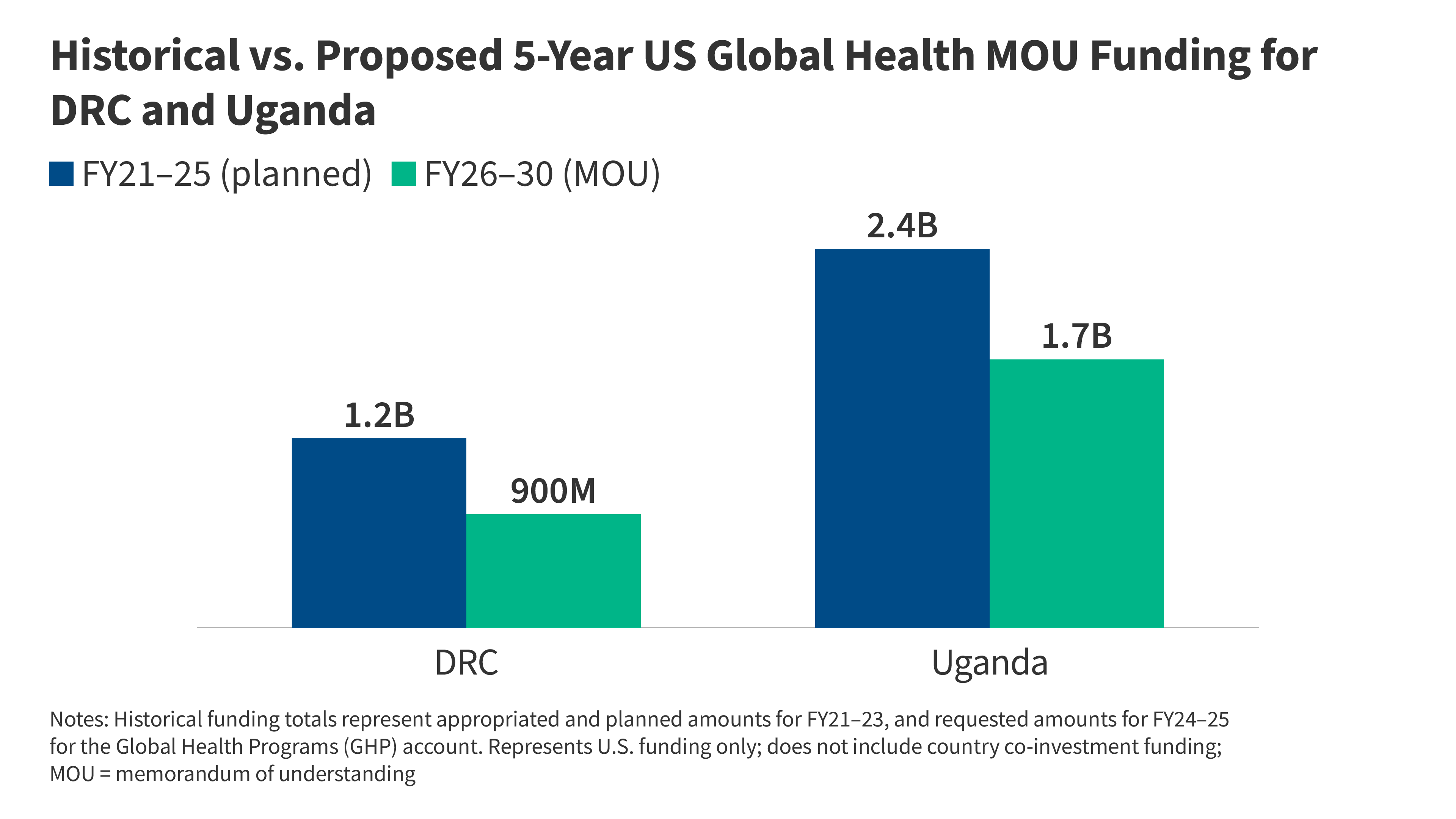
The "Historical vs. Proposed 5-Year US Global Health Funding" data, as analyzed by various health policy think tanks, suggests a significant contraction in long-term developmental support for the region. This reduction in foundational funding—money traditionally used to strengthen local healthcare systems—means that when an acute crisis like Ebola hits, the "baseline" health infrastructure is weaker than it was even five years ago.
Official Responses and Stakeholder Engagement
Despite the challenges, a broad coalition of organizations is mobilizing to stem the tide.
International and Local Coordination
The DRC and Ugandan ministries of health have assumed command of the response, supported by a sophisticated network of international actors:
- WHO: Leading the technical coordination and deploying rapid-response teams to manage laboratory diagnostics and case management.
- United Nations: Utilizing humanitarian channels to ensure food and resource security for affected communities under lockdown.
- Africa CDC: Playing a pivotal role in regional coordination, ensuring that data sharing between the DRC and Uganda remains transparent and actionable.
- NGOs: A coalition involving Médecins Sans Frontières (MSF), the International Rescue Committee (IRC), and CARE International are on the ground providing direct clinical care, community outreach, and psychosocial support.
The U.S. Response: A New Strategy
The U.S. government has announced a multi-pronged approach, but it differs fundamentally from past responses. Rather than leveraging centralized federal agencies as the primary engine for aid, the current response relies more heavily on private-sector partnerships and targeted, short-term grants. Critics argue that while this approach is fiscally leaner, it lacks the institutional depth and long-term continuity required to extinguish an Ebola outbreak, which often requires months of sustained surveillance and community engagement.
Implications: The Test of U.S. Global Leadership
The current outbreak is not merely a medical crisis; it is a geopolitical litmus test.
Key Questions for the Future
- Sustainability of Funding: Can the U.S. maintain its commitment if the outbreak extends beyond the current quarter, or will political fatigue lead to an early withdrawal of resources?
- The "America First" Dilemma: How effectively can the U.S. influence international health outcomes when its primary engagement strategy is built on bilateral, transactional agreements rather than the multilateral institutional support that characterized previous decades?
- Containment Efficacy: Does the current reliance on decentralized, NGO-led responses provide the same level of security against pathogen spread as the more integrated, government-led responses of the past?
A Comparative Perspective
Experts have noted that the domestic handling of recent health threats, such as the hantavirus, serves as a mirror to this international response. In both cases, the administration has opted for a "lean" response, prioritizing immediate, localized intervention over systemic, long-term capacity building. Whether this model can successfully contain a highly lethal, infectious, and geographically dispersed virus like Ebola remains the most pressing question in international public health today.
Conclusion: The Road Ahead
As the death toll rises and the infection footprint expands, the response to this outbreak will likely define the trajectory of global health security for the remainder of the decade. The swift, coordinated efforts of the WHO, African health authorities, and the NGO network demonstrate a high level of technical proficiency. However, the success of these frontline workers remains contingent upon the sustained, high-level political and financial backing of global powers.
If this crisis is contained, it will be a testament to the resilience of local health workers and the adaptability of international humanitarian organizations. If it spirals, it will serve as a stark warning about the risks of eroding the international health infrastructure. The world is watching, not just to see if the virus is defeated, but to see if the global community still possesses the architecture—and the political will—to act in concert against a common, invisible enemy. The weeks ahead will require more than just medical intervention; they will require a restoration of the global trust and cooperative mechanisms that have historically kept such existential threats at bay.