As of 2024, the United States is home to 24 million noncitizen immigrants, a demographic that encompasses both lawfully present individuals and the undocumented. While these individuals are foundational to the American workforce and economic stability, they increasingly find themselves navigating a precarious landscape regarding healthcare access. Driven by the 2025 federal budget reconciliation law and shifting state-level policies, the gap between the healthcare needs of immigrant families and their eligibility for coverage is widening, threatening long-term public health outcomes and economic productivity.
The Core Conflict: Federal Restrictions vs. Immigrant Health Needs
The U.S. healthcare system has long maintained a tiered approach to immigrant eligibility. Lawfully present immigrants, including green card holders, often face a mandatory five-year waiting period before becoming eligible for federal programs like Medicaid or the Children’s Health Insurance Program (CHIP). Undocumented immigrants are categorically excluded from all federally funded health coverage, including the Affordable Care Act (ACA) Marketplaces and Medicare.
The 2025 federal reconciliation law has further tightened these constraints. Starting October 1, 2026, the law restricts eligibility for Medicaid, CHIP, and subsidized Marketplace coverage almost exclusively to Lawful Permanent Residents (LPRs), specific humanitarian entrants (such as certain Cuban and Haitian arrivals), and citizens of Freely Associated (COFA) nations. Notably, the law eliminates ACA Marketplace subsidies for lawfully present immigrants with incomes below 100% of the Federal Poverty Level (FPL). For many refugees and asylees, these changes represent a significant loss of access to essential, federally supported medical care.
A Chronology of Policy Shifts (2025–2026)
The last eighteen months have marked a period of volatile policy adjustments:
- June 2025: The federal government issues regulations excluding DACA recipients from ACA Marketplace coverage, reversing earlier efforts to integrate this group into the private insurance market.
- Late 2025: The 2025 budget reconciliation law is signed, codifying strict new eligibility requirements for federal health programs and setting an October 2026 implementation date for most provisions.
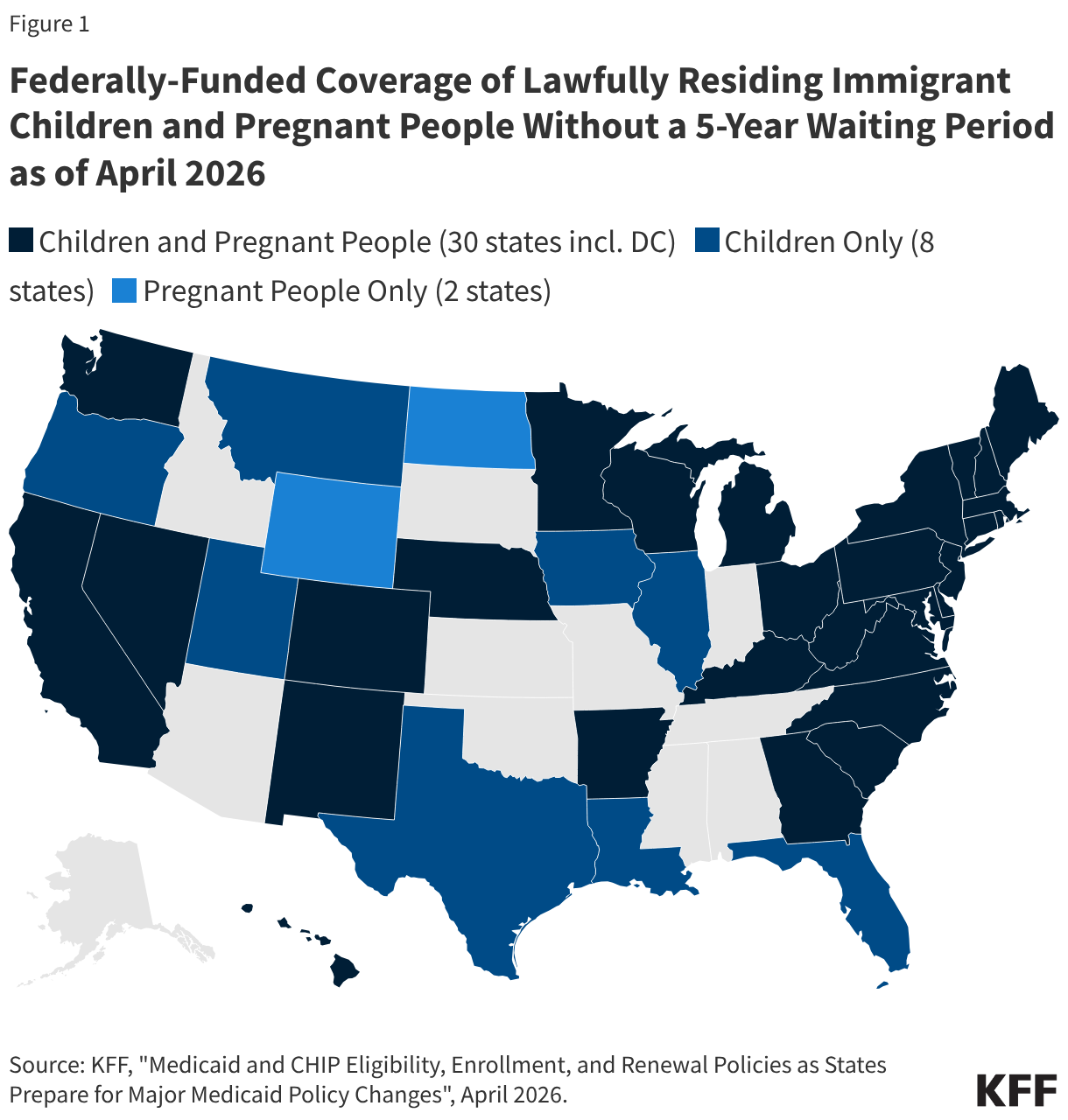
- April 2026: Assessment reveals that 38 states have adopted the Immigrant Children’s Health Improvement Act (ICHIA) option, while 25 states utilize the CHIP "From-Conception-to-End-of-Pregnancy" (FCEP) option to provide prenatal services.
- October 2026: The federal Medicaid matching rate for Emergency Medicaid services for "expansion adults" (those who would qualify but for their immigration status) is downgraded to the standard matching rate, placing a greater fiscal burden on states.
- Ongoing (2026): States like New Mexico and New York introduce legislation to create "bridge programs" to cover those displaced by federal cuts, while other states face intense budgetary pressure to scale back existing protections.
Supporting Data: The Impact of Coverage Gaps
The correlation between insurance status and health outcomes is stark. Research indicates that immigrant adults living in states with expansive coverage policies are nearly half as likely to be uninsured (11%) compared to those in restrictive states (23%).
The data further demonstrates that when states step in to fill the void, the results are immediate:
- Preventive Care: Children in states with universal coverage regardless of status are significantly less likely to forgo preventive dental or medical visits.
- Maternal Health: Expanding Medicaid to pregnant individuals regardless of immigration status is consistently associated with higher rates of prenatal care and superior birth outcomes.
- Economic Resilience: As highlighted by the KFF/New York Times 2025 survey, state-level expansions have successfully mitigated the "uninsurance penalty" for immigrant families, allowing them to remain productive members of the workforce rather than relying on high-cost, inefficient emergency room care.
The State Response: A Patchwork of Solutions and Retrenchment
Because the federal government has largely abdicated its role in covering undocumented immigrants and many lawfully present groups, states have become the primary laboratories for immigrant health policy.
The Rise of State-Funded Programs
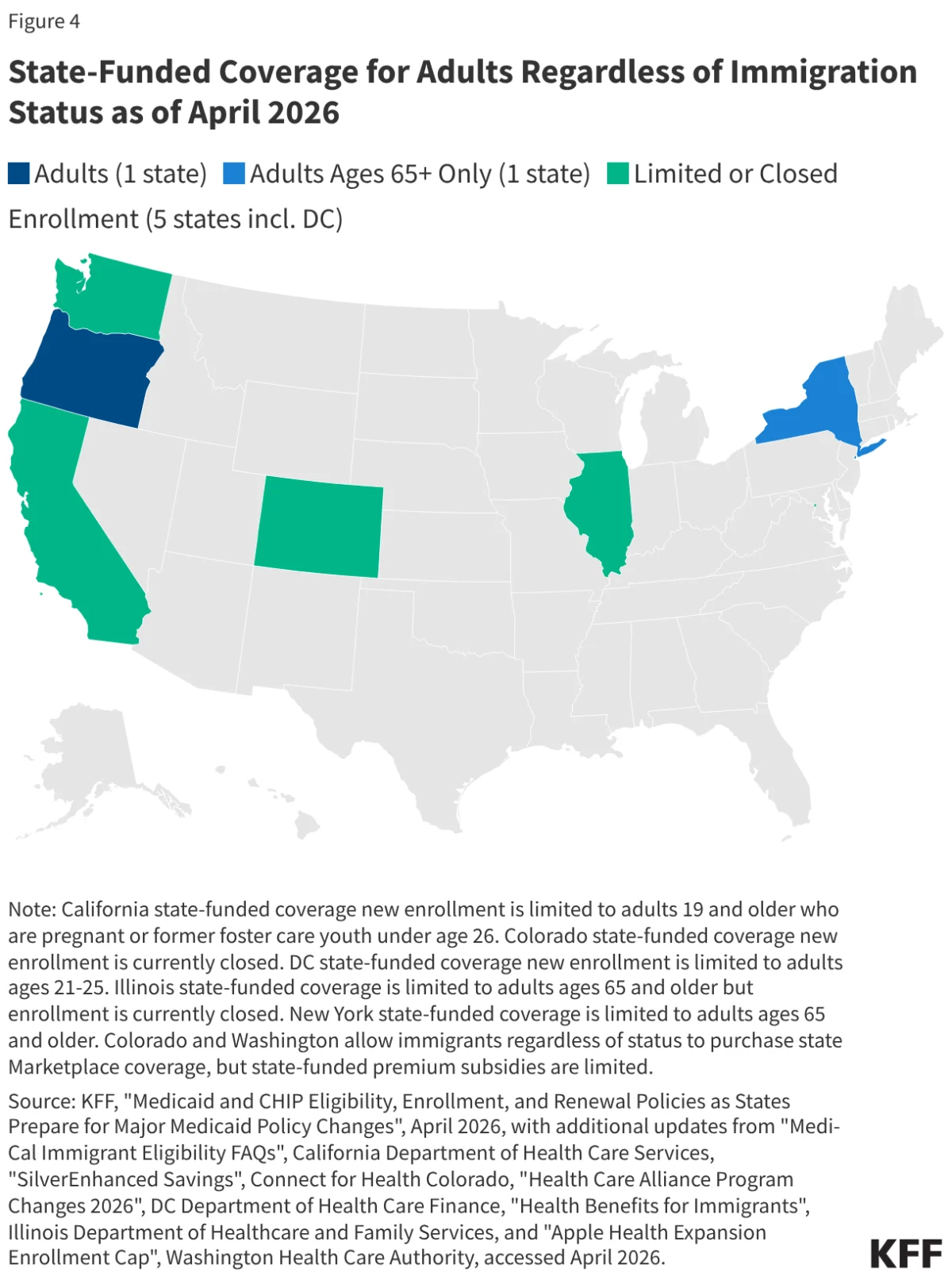
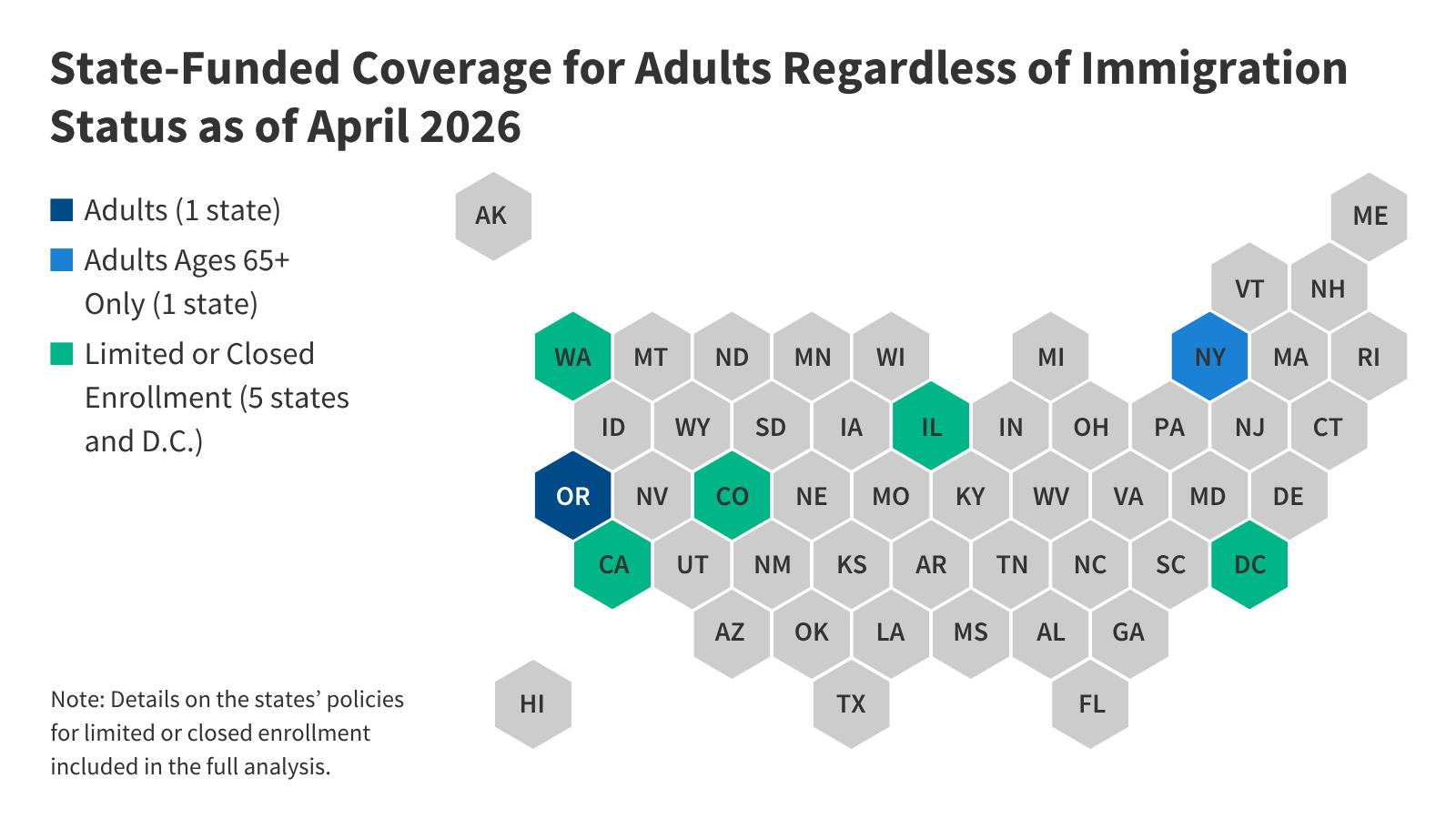
As of April 2026, 15 states—including California, Illinois, and New York—provide comprehensive state-funded coverage for children, regardless of immigration status. Seven states, including Washington and Oregon, have extended this coverage to specific populations of low-income adults. These programs act as a critical safety net, covering those in the "five-year wait" period or those who lack "qualified" status under federal definitions.
The Budgetary Crunch
Despite the clear health benefits, the fiscal reality is changing. Six states, including D.C., have recently reduced or eliminated state-funded coverage for adults due to budget shortfalls. Colorado, for example, has announced plans to cap enrollment and limit benefits for its children’s program starting in January 2027. Maryland has opted to delay the implementation of its marketplace expansion for undocumented individuals until 2028, citing the administrative burden caused by the 2025 federal reconciliation law.
Legislative "Bridge" Efforts
In response to the looming federal cuts, some states are actively seeking to protect their populations. New York’s current budget proposal aims to use state funds to cover those who lose their Essential Plan or Medicaid eligibility due to the 2025 federal law. New Mexico is similarly drafting legislation to cover DACA recipients and lawfully present immigrants affected by the federal changes. However, these efforts remain precarious, as they rely entirely on state tax revenues rather than federal matching funds.
Implications for the Future
The shift toward restrictive federal policy, coupled with state-level budgetary exhaustion, poses three significant risks to the United States:
1. The Erosion of Public Health
When immigrant families lose access to primary and preventive care, they do not simply stop getting sick. Instead, they delay care until conditions become acute. This leads to an increased reliance on emergency departments, which are the most expensive and least efficient settings for primary care. Emergency Medicaid spending, while currently a small fraction of total spending, may become a larger, more volatile cost center as states struggle to manage the influx of uninsured patients.

2. Long-term Economic Consequences
Immigrants are essential to sectors ranging from agriculture and construction to healthcare and technology. Unchecked health disparities result in lower workforce participation and decreased economic productivity. When parents cannot access care, they are more likely to miss work; when children lack access to school-based health services, their developmental and educational outcomes suffer.
3. The "State-Federal" Disconnect
The current trajectory threatens to create a "geography of health," where an immigrant’s access to life-saving care depends entirely on their state of residence. This creates an uneven landscape that undermines national health security. As states like North Carolina attempt to align their state laws with restrictive federal changes—even if such actions were, in some cases, unintentional—the confusion for both providers and patients creates an administrative barrier that is almost as damaging as the lack of funding itself.
Conclusion
The 2025 reconciliation law has fundamentally altered the terms of engagement for immigrant health. While states have historically served as a buffer against federal exclusion, the current economic climate is forcing many to withdraw from that role. Without a shift in federal policy or a sustainable, long-term approach to state-based funding, the United States faces a future of rising uninsured rates among vulnerable populations. The ultimate cost of this policy, however, will likely be paid in the form of poorer health outcomes for millions of residents and the erosion of a vital, productive segment of the American population.
Moving forward, policymakers must weigh the immediate budgetary savings of these restrictions against the long-term societal costs of a bifurcated, unequal, and inefficient healthcare system.