
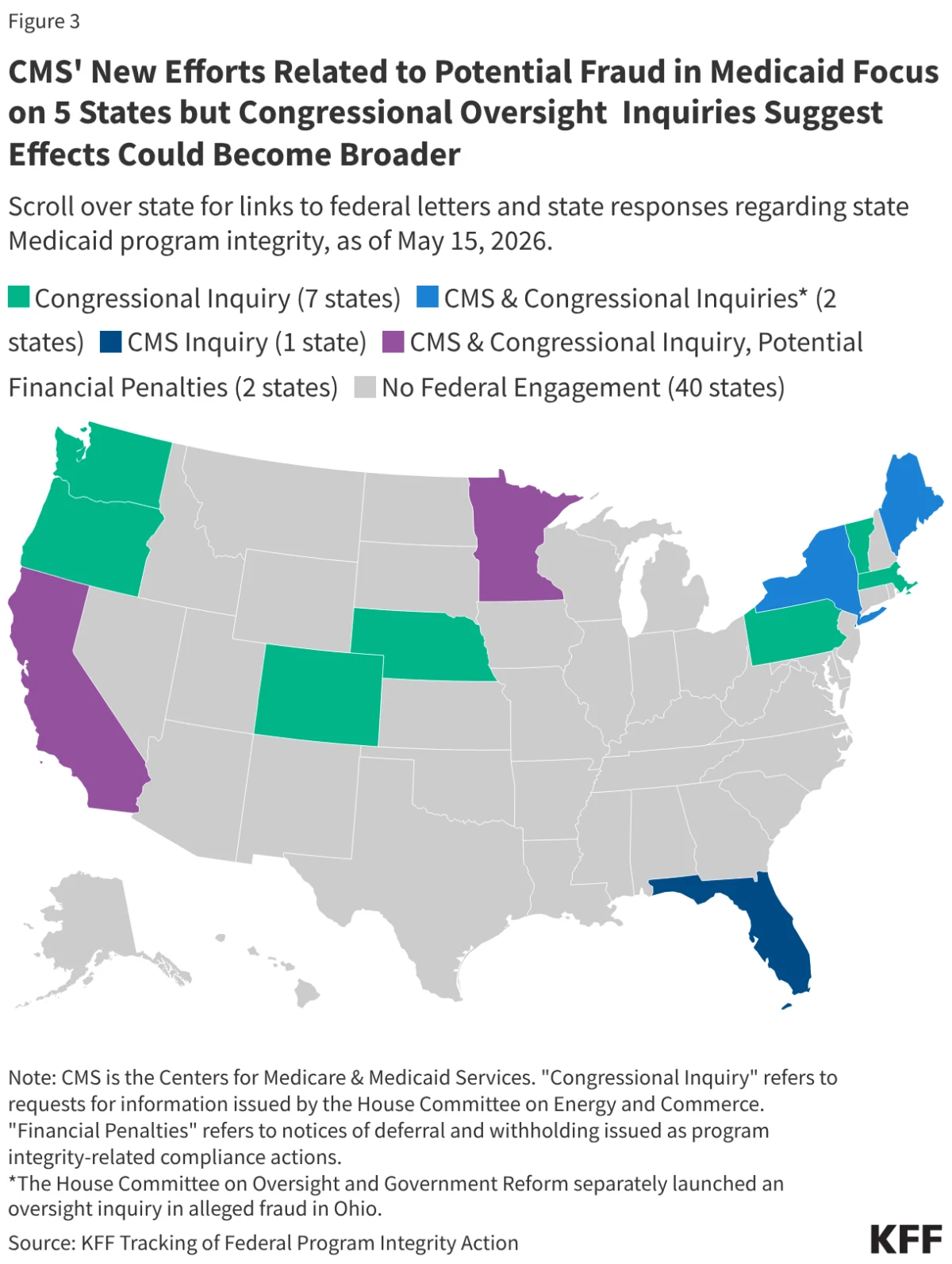
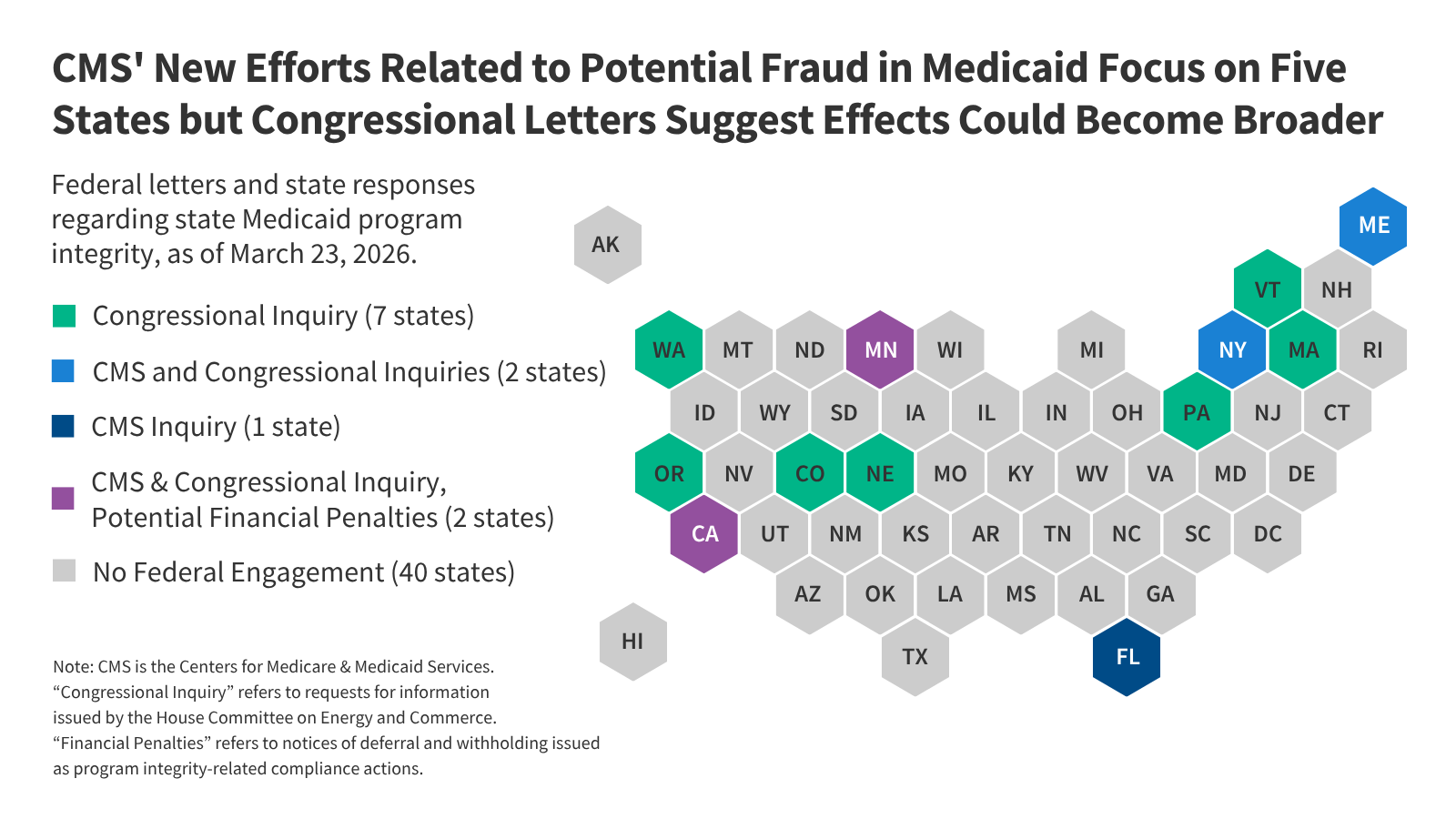
In a significant pivot in federal-state relations, the current administration has launched the "Comprehensive Regulations to Uncover Suspicious Healthcare" (CRUSH) initiative, a policy framework that marks a departure from historical methods of policing Medicaid expenditures. By shifting from reactive audits to proactive, large-scale financial interventions, the Centers for Medicare and Medicaid Services (CMS) is fundamentally altering how federal funds flow to state programs. This shift, which targets states with Democratic governors—specifically Minnesota, California, Maine, and New York—has sparked a national debate over the balance between program integrity and the fiscal stability of the healthcare safety net.
The Evolution of Federal Oversight: From Audits to Interventions
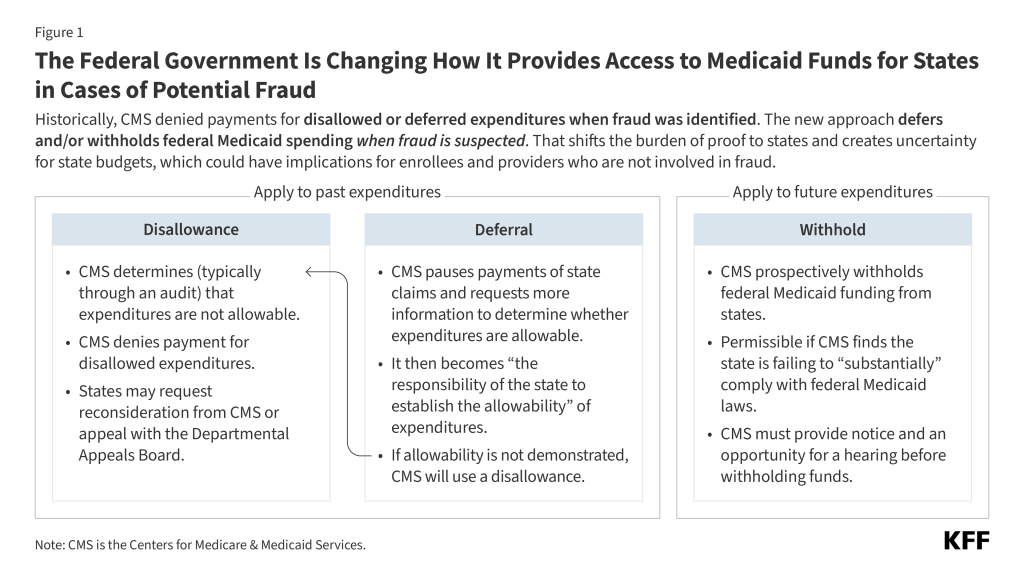
Historically, the relationship between CMS and state Medicaid programs has been rooted in a partnership model. When instances of fraud, waste, or abuse were detected, CMS typically engaged in a collaborative resolution process. If federal funds were found to be misspent, the agency would issue a "disallowance," retroactively denying the federal match for those specific expenditures.
However, under the CRUSH initiative, CMS is moving away from this retrospective approach. Instead, the agency is increasingly utilizing "deferrals" and "withholds" to proactively pause the flow of federal dollars based on suspicions of fraud, even before a definitive investigation has concluded. This strategy forces states to carry the burden of proof, requiring them to demonstrate the "allowability" of their expenditures while their budgets are effectively frozen.
Chronology of the CRUSH Initiative (2025–2026)
- Late 2025: The administration signals a shift toward aggressive Medicaid oversight, citing concerns over rising improper payments and potential systemic fraud.
- January 13, 2026: Minnesota formally requests a hearing after being notified that CMS plans to withhold $515 million in quarterly federal Medicaid payments.
- January 14, 2026: Official federal notification is sent to Minnesota, detailing the intent to withhold funds pending the outcome of a compliance hearing.
- January 30, 2026: Minnesota submits a revised Corrective Action Plan (CAP) to CMS, aiming to satisfy federal integrity requirements.
- March 20, 2026: CMS accepts Minnesota’s revised CAP, providing a temporary reprieve from the withholding process, provided the state meets its milestones.
- March 25, 2026: By this date, four additional states have received formal letters from CMS requesting detailed information regarding their program integrity measures.
- May 15, 2026: Most recent update to the federal brief tracking ongoing actions against states regarding potential Medicaid fraud.
Understanding the Financial Tools: Disallowances, Deferrals, and Withholds
To understand the gravity of this shift, one must distinguish between the three primary financial mechanisms CMS employs to police the program.
The Disallowance: The Traditional Hammer
A disallowance occurs after a state has already spent federal money on a claim that is later deemed ineligible. The state is then required to return those funds. Because this happens after the fact, the administrative process—including appeals to the Departmental Appeals Board—can take over a decade to resolve. Historically, this tool was reserved for well-documented cases of clear-cut fraud.
The Deferral: The Immediate Pause
A deferral acts as an immediate stop-gap. CMS pauses payment for expenditures that have already occurred while demanding that the state provide documentation to prove the costs were legitimate. If the state cannot provide sufficient evidence within a strict 90-day window, the deferral converts into a permanent disallowance. In early 2026, the administration deferred a record-breaking $259 million in federal payments to Minnesota, setting a precedent for the scale at which this tool might now be used.
The Withhold: The Compliance Weapon
The most severe tool in the arsenal is the "withhold." Unlike a deferral, which relates to specific claims, a withhold targets the funding stream itself, often because a state is deemed to be in "non-compliance" with federal law. While previous administrations used withholdings sparingly—usually involving 1% to 10% of specific administrative budgets—the current proposal for Minnesota involved nearly 20% of its annual federal share. This level of withholding threatens the operational solvency of state Medicaid programs.
Supporting Data and Congressional Oversight
The reach of the CRUSH initiative extends beyond executive action. The House Committee on Energy and Commerce has escalated its oversight role, sending formal inquiries to 11 states. These inquiries are not limited to the four states currently under the microscope of CMS.
Publicly available data on Medicaid expenditures, while lacking specific line-item detail regarding fraud-related adjustments, confirms that federal-state financial volatility is increasing. Between 2020 and 2025, the Departmental Appeals Board issued 12 rulings on Medicaid disallowances. In the six cases where new rulings were made, the average time elapsed between the disputed expenditure and the final decision was 15 years. This highlights a critical flaw in the system: if the federal government continues to rely on these mechanisms, states could be locked in multi-year litigation while their funding remains in limbo.
Official Responses and State Perspectives
State officials and the National Association of Medicaid Directors (NAMD) have expressed significant concern. The primary argument from the states is that the CRUSH initiative punishes entire state programs for localized issues. Because states are legally required to maintain balanced budgets, the sudden loss of federal matching funds creates an immediate liquidity crisis.
NAMD has advocated for a more constructive partnership, proposing that CMS focus on:
- Technical Assistance: Providing states with better data-sharing capabilities to identify fraud before it occurs.
- Modernized Fraud Detection: Investing in advanced analytics rather than aggressive, high-stakes funding freezes.
- Collaborative Resolution: Establishing clearer, faster pathways for resolving disputes that do not threaten the delivery of care to vulnerable populations.
Implications for Enrollees and Healthcare Providers
The most profound impact of the CRUSH initiative is the potential for collateral damage. When federal funding is withheld or deferred, states are forced into a corner. To maintain a balanced budget, a state may be forced to:
- Reduce Provider Rates: Reducing reimbursement to doctors and hospitals can lead to decreased access to care, particularly in rural or underserved areas where Medicaid is the primary payer.
- Restrict Coverage: States might be forced to limit the types of services covered or tighten eligibility requirements to compensate for the lost federal match.
- Administrative Burden: The sheer volume of audits and documentation required by the CRUSH initiative imposes a heavy burden on providers, who must now spend more time on paperwork and less time on patient care.
The Intersection with 2025 Reconciliation Law
This new approach to fraud does not exist in a vacuum. It is unfolding simultaneously with the implementation of the 2025 reconciliation law, which enacted historic reductions in federal Medicaid spending and introduced complex new work requirements for expansion enrollees.
States are already struggling to overhaul their administrative systems to comply with these new federal mandates. Adding the CRUSH initiative’s aggressive posture creates a "double-squeeze" effect. States are being asked to implement complex new policies while their financial foundations are being destabilized by federal funding pauses. The cumulative effect of these policies is an environment of profound uncertainty, where the stability of the Medicaid program—and the health security of millions of low-income Americans—depends on the resolution of complex, high-stakes administrative battles.
As of May 2026, the situation remains fluid. While Minnesota has managed to secure a pathway forward through an accepted corrective action plan, the broader implications for the 11 states under congressional investigation and the four states under the CMS spotlight suggest that the era of aggressive Medicaid policing has only just begun. The long-term success of this initiative will likely be measured not by the amount of funds recovered, but by the stability of the safety net that remains when the dust settles.






