By Medical Science Correspondent
Laryngeal squamous cell carcinoma (LSCC) remains a formidable challenge in modern oncology, characterized by high rates of morbidity and complex clinical behavior that often defies traditional staging methods. A groundbreaking study published in the journal Diagnostics (2026) has shed new light on this malignancy, moving beyond simple anatomical classification to reveal how the tumor’s internal immune environment dictates patient survival. By identifying three distinct "immune patterns," researchers have provided a new framework for predicting outcomes and potentially tailoring future therapeutic interventions.

Main Facts: The Immune Microenvironment as a Prognostic Compass
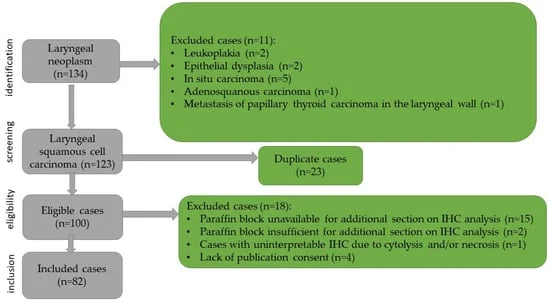
The study, led by a multidisciplinary team from the "Victor Babeș" University of Medicine and Pharmacy in Timișoara, Romania, investigated 82 patients diagnosed with LSCC. While conventional histopathology—such as tumor grade and size—has long been the standard for clinical decision-making, it often fails to account for the dramatic differences in how patients respond to the same treatment protocols.
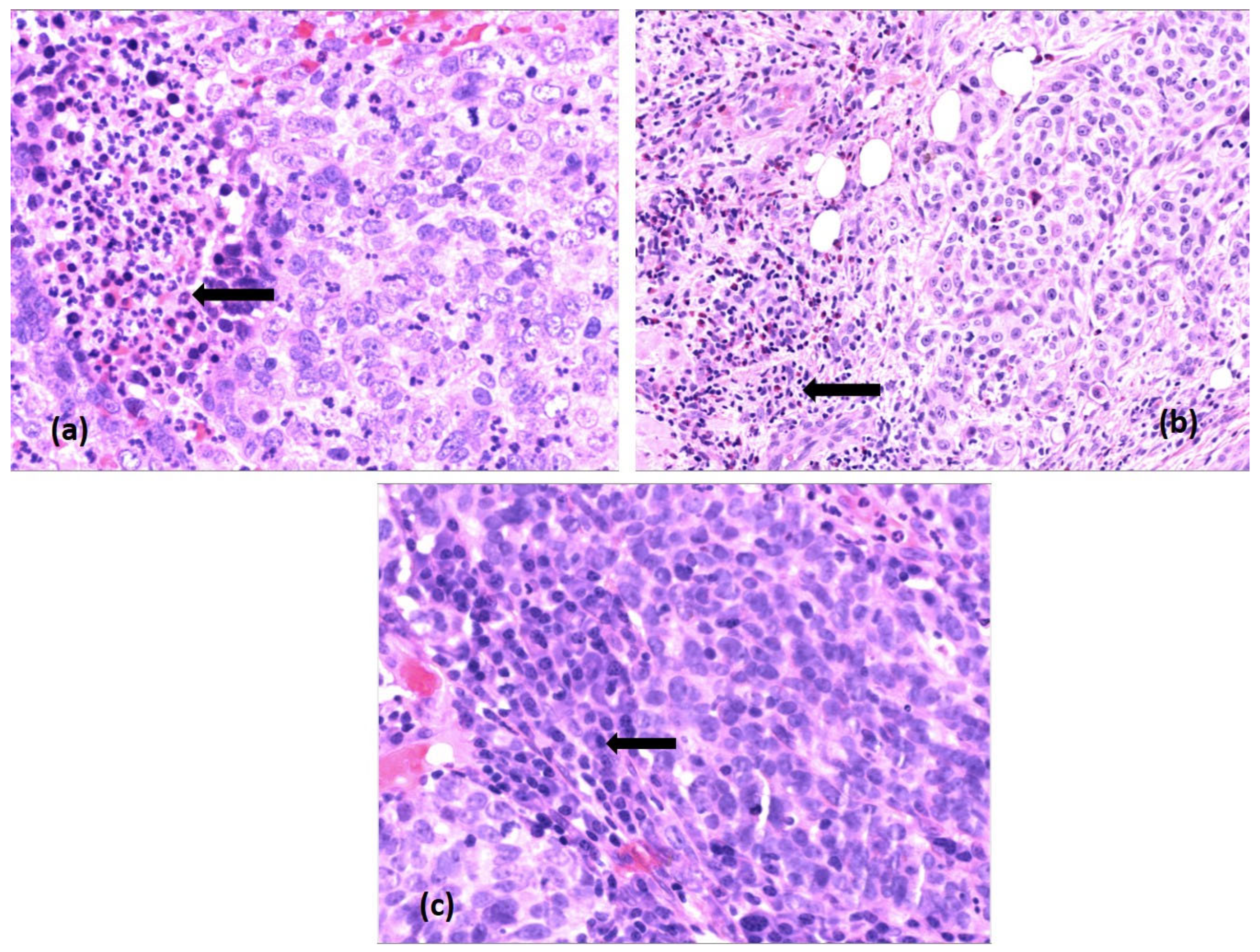
The researchers focused on the Tumor Immune Microenvironment (TME), a complex ecosystem comprising immune cells, stromal components, and the extracellular matrix. By utilizing an extensive immunohistochemical panel, the team quantified the density of various immune cells, including B lymphocytes (CD20+), T lymphocytes (CD3+, CD4+, CD8+), macrophages (CD68+), dendritic cells (CD1a+), and mast cells (CD117+).
The core finding is the classification of these tumors into three specific "Immunotypes":
- Immunotype A (Active Immune Type): Characterized by a dense infiltration of effector T cells and B cells. These patients showed the most favorable clinical outcomes.
- Immunotype B (Mixed Type): Exhibiting intermediate, heterogeneous immune cell distribution, representing a middle ground in prognostic risk.
- Immunotype C (Immunosuppressive Type): Defined by a scarcity of effector immune cells and a high prevalence of regulatory elements like macrophages and mast cells. These patients faced the poorest survival rates.
Chronology of the Study
The research represents a rigorous, long-term observation effort spanning nearly a decade of patient care and data analysis:

- January – December 2018: The recruitment phase for the retrospective cohort. 82 patients were admitted to the Otorhinolaryngology Department of the Timișoara City Emergency Hospital, receiving initial histopathological confirmation of LSCC.
- 2018 – 2025: An eight-year longitudinal follow-up period. Patients were monitored for recurrence, metastasis, and mortality, with data cross-referenced via the Central Population Registry.
- March 2022: Formal initiation of the research protocol and ethical approval obtained from the institutional committee.
- March 13, 2026: Submission of the formal research manuscript to Diagnostics.
- April 2026: Peer review and revisions completed, followed by formal acceptance of the study.
- May 8, 2026: Final publication, providing the scientific community with a new model for risk stratification in head and neck cancers.
Supporting Data: The Statistical Weight of Immunity
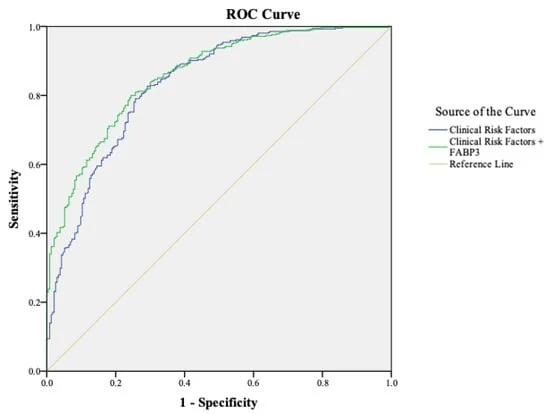
The strength of the study lies in its statistical validation. The researchers employed Kaplan-Meier survival curves to compare the three immunotypes, and the differences were stark.
Patients classified under Immunotype A demonstrated a 5-year overall survival rate of 91.7%, compared to just 12.1% for those with Immunotype C. The findings remained statistically significant even when adjusted for traditional clinicopathologic factors like tumor stage (pT), nodal involvement (pN), and vascular invasion.

In multivariable Cox regression models, the hazard ratio for death was 24.79 times higher for patients with Immunotype C compared to those with Immunotype A. Furthermore, the study noted a significant correlation between p16 status—a common surrogate marker for HPV infection—and the immune profile. All p16-positive tumors were found to be of the "Active" Immunotype A, reinforcing the link between viral-associated cancers and a more robust immune response.
Official Perspective and Methodological Rigor
The research team, which included experts from departments of pathology, ear-nose-throat, and emergency medicine, emphasized that their work is not merely about identifying individual markers, but about the integration of these markers into a holistic profile.
"The novelty of this work lies not in the analysis of single markers per se but in the identification of immune pattern-based subtypes," the authors noted. By using a semiquantitative scoring system (0 to 3), the team ensured that the classification was both reproducible and clinically actionable.
The study also addressed the role of innate immune cells. While neutrophils and mast cells are often overlooked, the study found that high densities of mast cells in the immunosuppressive (Type C) tumors correlated with poorer outcomes, suggesting that these cells may play a pro-tumorigenic role in the laryngeal environment. However, the authors were careful to state that these observations are correlative, and further mechanistic research is required to determine if these cells directly drive tumor progression or are simply markers of an already aggressive environment.

Clinical Implications: A New Era for LSCC Management
The implications of this research are potentially transformative for the treatment of laryngeal cancer. Currently, treatment plans are largely dictated by the TNM staging system (Tumor, Nodes, Metastasis). While effective, this system is purely anatomical and does not account for the biological "personality" of the tumor.
1. Refined Risk Stratification
By incorporating "Immunotype" into the initial biopsy report, clinicians could identify high-risk patients who might require more aggressive adjuvant therapies, even if their tumor stage is considered "early" by traditional measures.

2. Tailored Immunotherapy
The findings support the growing push for immunotherapy in head and neck cancers. Patients with "Immunotype C" (immunosuppressive) profiles might be primary candidates for clinical trials testing immune checkpoint inhibitors, which aim to "wake up" the immune system in the presence of these inhibitory cells.
3. Future Research Directions
The authors acknowledge several limitations, including the small sample size and the reliance on immunohistochemistry rather than molecular techniques like RNA sequencing. Nevertheless, the study provides a robust baseline for future multicenter trials. "These observations remain exploratory," the authors concluded, "and require validation in larger, independent cohorts before any clinical application can be considered."

4. Patient Quality of Life
For patients, the ultimate goal of such research is the preservation of laryngeal function. By better understanding the TME, doctors may be able to choose less invasive surgeries (like laser cordectomy) for patients identified with "active" immune profiles who have a lower risk of recurrence, thereby sparing the patient from the functional deficits associated with total laryngectomy.
As the field of immuno-oncology continues to evolve, studies like this from the University of Medicine and Pharmacy "Victor Babeș" serve as a vital reminder that the battle against cancer is fought not just by the surgeon’s blade, but by the patient’s own biological defenses. The ability to "read" the tumor’s immune signature is a significant step toward a future where cancer treatment is as unique as the immune system of the person fighting it.