By Medical Science Correspondent
In the complex field of esophageal cancer surgery, the procedure of esophagectomy remains a formidable challenge. While surgical techniques have evolved significantly, one complication has remained a persistent threat to patient recovery: cervical anastomotic leakage (AL). A recent study published in the journal Cancers (2026) offers a potential breakthrough in managing this risk. Researchers at the National Cancer Center Hospital in Tokyo have demonstrated that a simple, reproducible refinement—staple-line oversewing—can significantly improve patient outcomes following a Totally Mechanical Collard (TMC) cervical anastomosis.

Main Facts: A Shift in Surgical Protocol
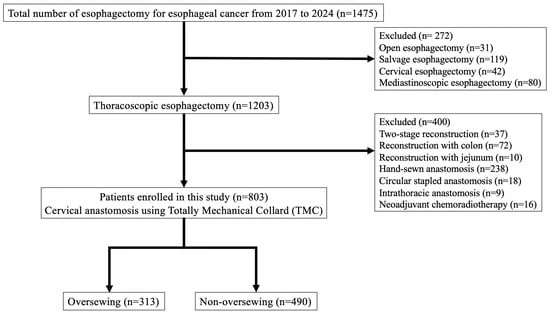
The study, led by Dr. Koshiro Ishiyama and his team, analyzed 803 consecutive patients who underwent esophagectomy with cervical esophagogastric reconstruction between 2017 and 2024. The research compared two distinct cohorts: 490 patients who underwent standard TMC anastomosis and 313 patients who received the additional “staple-line oversewing” modification.
The findings were statistically significant. The group that received the reinforcing sutures experienced a notably lower incidence of anastomotic leakage (4.4%) compared to the non-oversewing group (8.1%). Beyond the raw incidence rates, the study highlighted that when leaks did occur in the oversewing group, they were typically less severe. The reinforcement technique was achieved using 4-0 Vicryl sutures to invert and reinforce the posterior and anterior edges of the staple line, a maneuver that the authors argue adds a vital layer of mechanical stability to the reconstructed esophagus.
Chronology of the Study
The research period spanned eight years, reflecting a transition in standard practice at the National Cancer Center Hospital.
- 2017–2020 (Baseline Period): During this initial phase, the surgical department routinely performed the non-oversewing TMC anastomosis. This period provided a robust control group of 490 patients.
- 2021 (Institutional Change): Recognizing the variable nature of leakage rates and the potential for mechanical failure, the institution officially introduced routine staple-line oversewing as part of their standard operative protocol.
- 2021–2024 (Intervention Period): The team implemented the new technique across 313 patients. Throughout this period, data was meticulously collected, categorized, and compared against the historical control group.
- April–May 2026: The study underwent peer review, was accepted for publication on May 7, 2026, and was officially released on May 8, 2026, providing the medical community with clear evidence for the efficacy of the technique.
Supporting Data and Statistical Analysis
To ensure the validity of their findings, the researchers conducted a multivariable logistic regression analysis. This statistical approach allowed them to isolate the impact of the oversewing technique from other potential variables, such as patient age, smoking status, pulmonary function, and intraoperative blood loss.

The results of this analysis identified two primary independent risk factors for anastomotic leakage: a body mass index (BMI) of 25 kg/m² or greater, and the absence of staple-line oversewing. Patients in the non-oversewing group were more than twice as likely (OR 2.15) to experience leakage.
Crucially, the study addressed a common concern among surgeons: whether adding sutures would increase the risk of anastomotic stricture—a narrowing of the opening that can cause long-term swallowing difficulties. The data provided reassurance; the incidence of strictures remained low and did not differ significantly between the two groups (3.5% in the oversewing group vs. 5.3% in the non-oversewing group, p = 0.3). Furthermore, the oversewing group showed lower rates of other postoperative complications, including pneumonia and vocal cord paralysis, suggesting that the technique may contribute to a safer, more stable overall postoperative recovery.

Official Perspectives and Expert Insight
The research team emphasized that the success of the oversewing technique lies in its mechanical simplicity. In their discussion, the authors noted: “Staple-line oversewing may improve the safety and stability of cervical esophagogastric anastomosis after esophagectomy.”
Dr. Ishiyama and his colleagues point out that while various techniques, such as hand-sewn or circular-stapled anastomoses, have been utilized for years, the linear-stapled TMC approach is favored for its wider lumen. However, the tension generated during conduit elevation and the early stages of swallowing can stress the staple line. The additional sutures act as a buffer, distributing this stress more evenly across the tissues.

One of the most compelling aspects of the data is the change in the clinical course of leaks. In the oversewing group, Grade I (minor) leaks were significantly more frequent, while more severe, cavity-forming leaks were less common. Additionally, the onset of leakage was delayed in the oversewing group. The authors suggest that this delay might be due to the improved early mechanical integrity of the anastomosis, allowing patients more time to develop protective adhesions around the site, which in turn limits the severity of any potential infection.
Clinical Implications for Future Practice
The implications of this study are twofold for the field of thoracic and esophageal surgery.

1. Standardization of Care
The study suggests that hospitals performing high-volume esophageal cancer surgeries might benefit from adopting a standardized, routine approach to staple-line reinforcement. Because the technique is "simple and reproducible," it does not require expensive new equipment or specialized training, making it an accessible upgrade for surgical departments globally.
2. A Call for Prospective Validation
While the researchers are encouraged by the outcomes, they remain scientifically rigorous, noting that the study’s retrospective design and the temporal overlap with the rise of robot-assisted surgery—which also became more frequent during the study period—could introduce confounding factors.

"This study should be considered hypothesis-supporting rather than definitive," the authors stated in their conclusion. They have called for a prospective, multicenter registry to further validate these findings and to confirm whether this technique should become the new international "gold standard" for TMC cervical anastomosis.
As the global medical community continues to refine minimally invasive approaches to cancer, findings like these serve as a reminder that even incremental changes in surgical technique can lead to substantial improvements in patient morbidity and quality of life. By focusing on the mechanical stability of the esophageal reconstruction, surgeons can move closer to the goal of making complex esophagectomies safer, more predictable, and less burdensome for patients recovering from cancer.