The landscape of American healthcare is undergoing a profound transformation, yet for millions of seniors and individuals with disabilities, this transition is increasingly defined by a singular, frustrating obstacle: the "prior authorization" wall. As Medicare Advantage (MA) plans continue to dominate the federal health insurance market—now enrolling more than half of all Medicare beneficiaries—the mechanisms these private insurers use to manage care have come under intense public and regulatory scrutiny.
Recent investigations by the Department of Health and Human Services’ Office of Inspector General (OIG) have cast a spotlight on a systemic pattern of denials for post-acute care services, suggesting that the very tools designed to reduce "low-value" care may be creating significant barriers for the most vulnerable patients.
The Core Conflict: Managing Costs vs. Patient Access
Prior authorization—a process requiring healthcare providers to obtain pre-approval from an insurer before a service is covered—has long been framed by the insurance industry as a necessary check against overutilization. By curbing unnecessary procedures and controlling costs, insurers argue they are maintaining the fiscal sustainability of the Medicare program.
However, a KFF polling analysis reveals a growing disconnect between these administrative goals and the patient experience. Approximately seven in ten insured adults now view prior authorization as a significant burden. When these bureaucratic hurdles are applied to life-critical post-acute services, the implications shift from mere inconvenience to potential health risks.
Chronology of the Regulatory Crackdown
The current climate of scrutiny is the result of a multi-year trend that has caught the attention of federal oversight bodies and legislative investigators:
- 2019–2022: During this period, a U.S. Senate investigation identified a consistent pattern among the nation’s largest Medicare Advantage organizations. The inquiry revealed that these insurers were denying prior authorization requests for post-acute care at rates substantially higher than for other medical services.
- 2024: Medicare Advantage insurers reached a staggering milestone, processing nearly 53 million individual prior authorization determinations. This volume highlighted the sheer scale of the administrative apparatus managing senior care.
- Late 2024/Early 2025: Several private insurers made public pledges to streamline their prior authorization processes, responding to mounting pressure from the Centers for Medicare & Medicaid Services (CMS) and public advocacy groups.
- 2026: The OIG released two landmark reports documenting the specific failure points in the system, particularly regarding long-term acute care and rehabilitation, confirming the fears raised by earlier legislative probes.
Supporting Data: The Disparity in Denials
The OIG’s latest findings provide the most damning evidence to date regarding the disparity between standard medical necessity determinations and the realities of post-acute care management.
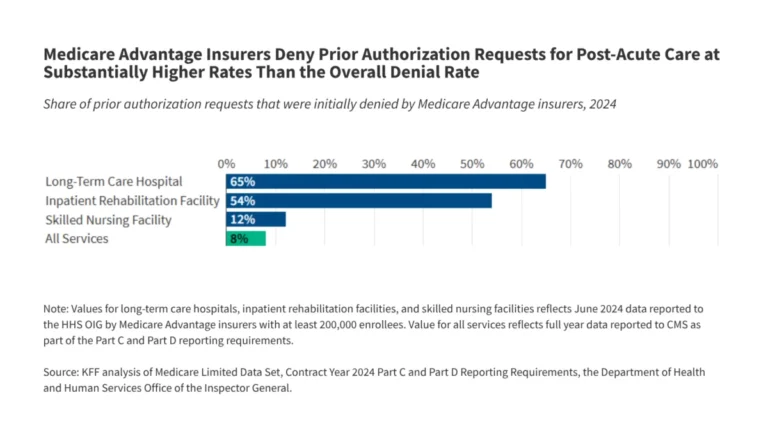
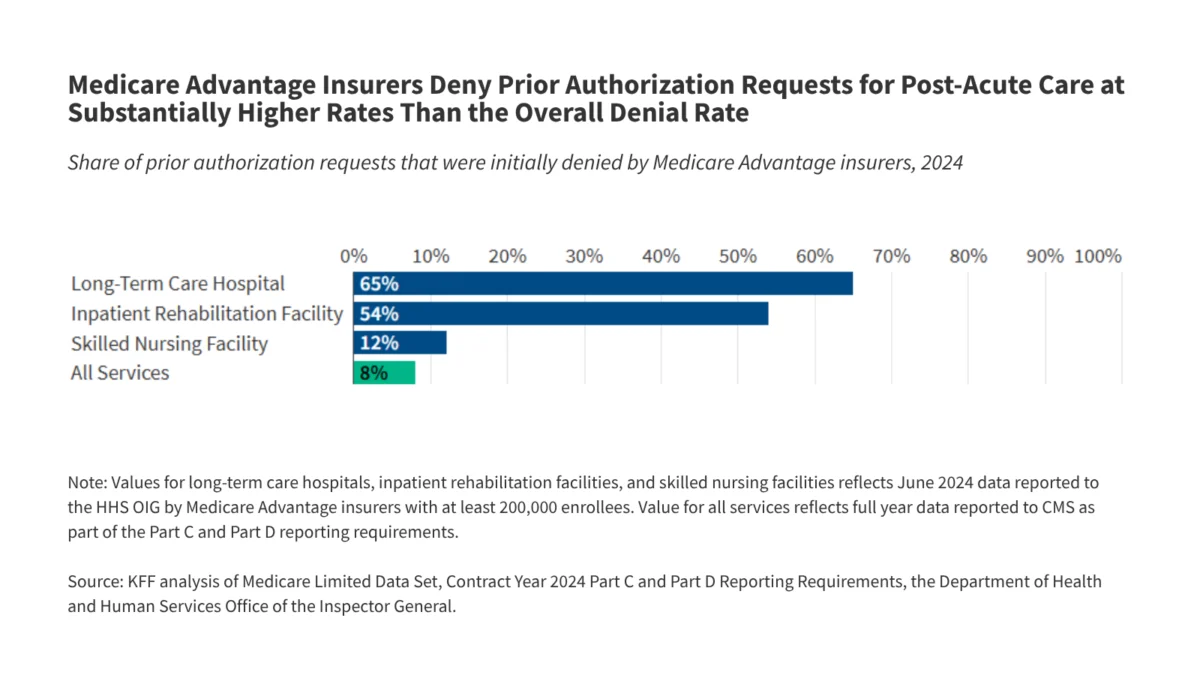
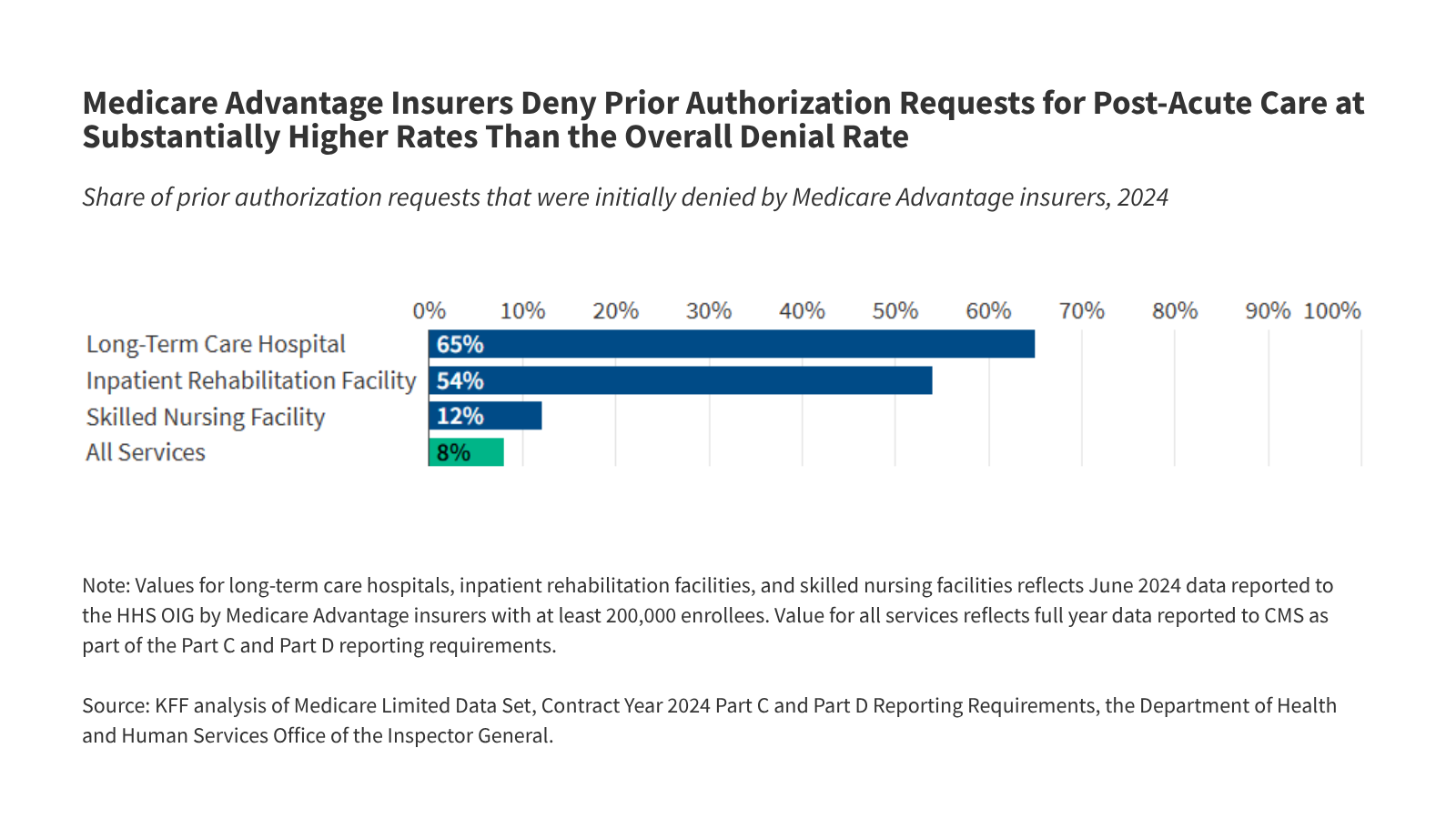
While the average Medicare Advantage prior authorization denial rate for all services sits at roughly 8%, the rates for high-cost, high-acuity post-acute care are dramatically higher:
- Long-Term Acute Care Hospitals (LTCHs): 65% of requests denied.
- Inpatient Rehabilitation Facilities (IRFs): 54% of requests denied.
- Skilled Nursing Facilities (SNFs): 12% of requests denied.
The financial stakes are immense. According to the Medicare Payment Advisory Commission (MedPAC), the average cost per stay for these services is significant: $43,000 for an LTCH stay, $24,000 for an IRF, and $16,000 for a skilled nursing facility. By denying these requests, insurers are effectively gatekeeping access to tens of thousands of dollars in care.
Perhaps most alarming is the data surrounding appeals. When these denials are challenged, the success rate for the patient or provider is profound. For skilled nursing facilities, a staggering 95% of initial denials are overturned upon appeal. For IRFs, 43% are reversed, and for LTCHs, 36% are overturned. These figures suggest that a large proportion of initial denials are, by the insurer’s own admission, erroneous or unsupported by clinical reality.
The Human and Clinical Implications
The consequences of these denials extend far beyond the balance sheet. Patients requiring LTCH or IRF services are often in fragile condition, recovering from strokes, brain injuries, or managing multiple chronic comorbidities requiring specialized respiratory or pain management.
The OIG found that an initial denial leads to a delay in care averaging between five and six days. For a patient waiting to transition from a hospital to a rehabilitation center, these days are not merely idle; they are periods of clinical stagnation. Furthermore, these delays often translate into direct financial penalties for the patient. Because many Medicare Advantage plans impose daily cost-sharing requirements for hospital stays, a delay caused by a denied authorization can result in the patient incurring thousands of dollars in unexpected out-of-pocket costs while they sit in an acute-care bed awaiting a transfer that should have been authorized immediately.
Why the High Overturn Rate?
The high rate of overturned denials—particularly the 95% reversal for skilled nursing facility requests—raises a critical question: Are these denials the result of simple administrative error, or is there an intentional strategy at play?
Industry analysts suggest a phenomenon known as "the deterrent effect." If an insurer knows that only a small percentage of patients (or their providers) have the resources and stamina to navigate the complex appeals process, they may systematically deny claims, knowing that a significant portion will never be challenged.
However, there is a secondary layer of risk for the insurers. If an appeal proceeds to the final stage, it is reviewed by an Independent Review Entity (IRE). If the IRE consistently finds that an insurer’s denial was improper, that data can trigger a negative impact on the plan’s "Star Rating." By overturning their own denials early in the appeals process, insurers may be effectively "buying off" the complaint to avoid the scrutiny of an external audit.
Official Responses and the Data Transparency Gap
The lack of granular, service-level data has long been the insurance industry’s best defense against regulation. Because insurers were not historically required to report detailed, standardized metrics on why specific claims were denied, it has been nearly impossible for regulators to perform an apples-to-apples comparison of plan performance.
CMS has acknowledged this gap and is moving to close it. A new pilot program aimed at collecting detailed, service-level data is currently underway. CMS anticipates that it will be able to mandate comprehensive reporting by 2027. However, health policy experts warn that this timeline is too slow given the rapid expansion of the Medicare Advantage program.
"The current system relies on a ‘trust us’ model that is clearly failing the most vulnerable," says one healthcare policy analyst. "Without real-time data transparency, we are flying blind while patients are being denied the care they are entitled to."
Moving Toward Reform
The path forward involves a delicate balance. Insurers maintain that they provide a service to the Medicare program by identifying and eliminating waste. However, the OIG reports have provided the hard evidence necessary to shift the conversation from "whether" to "how" the system must be regulated.
Proposed reforms include:
- Standardized Criteria: Establishing federal, evidence-based clinical guidelines that all MA plans must follow, preventing the current "heterogeneous experience" where coverage depends entirely on which private insurer the enrollee chose.
- Automated Appeals: Streamlining the appeals process so that if a clinician provides evidence that meets standard criteria, the override is automatic rather than manual.
- Increased Penalties: Aligning Star Ratings more closely with denial/overturn rates, ensuring that plans that routinely deny valid care face immediate and significant financial consequences.
As the Medicare Advantage program continues to age, the pressure to prove that it provides equal or better value than traditional Medicare will intensify. For now, the administrative wall of prior authorization remains the most significant barrier to that promise. Until the data is transparent and the denial rates for post-acute care are brought in line with clinical reality, the burden of proof—and the burden of suffering—will continue to rest on the shoulders of the patients.