The landscape of Medicaid and the Children’s Health Insurance Program (CHIP)—the safety net providing essential health coverage to millions of low-income Americans—is undergoing its most significant transformation in a decade. As of March 2026, the national enrollment figures reflect a system that has transitioned from the unprecedented expansion of the COVID-19 pandemic era into a new phase of federal oversight, legislative reform, and rigorous eligibility re-evaluation.
Following the conclusion of the pandemic-era "continuous enrollment" provision, the United States is currently navigating the long-term aftermath of a massive administrative "unwinding." This report synthesizes the latest data from the Centers for Medicare & Medicaid Services (CMS) and independent analysis to provide a clear picture of how enrollment patterns are shifting, what the new legislative requirements mean for the future of the program, and how the stability of coverage is being redefined in the post-pandemic era.
Main Facts: The Current State of Enrollment
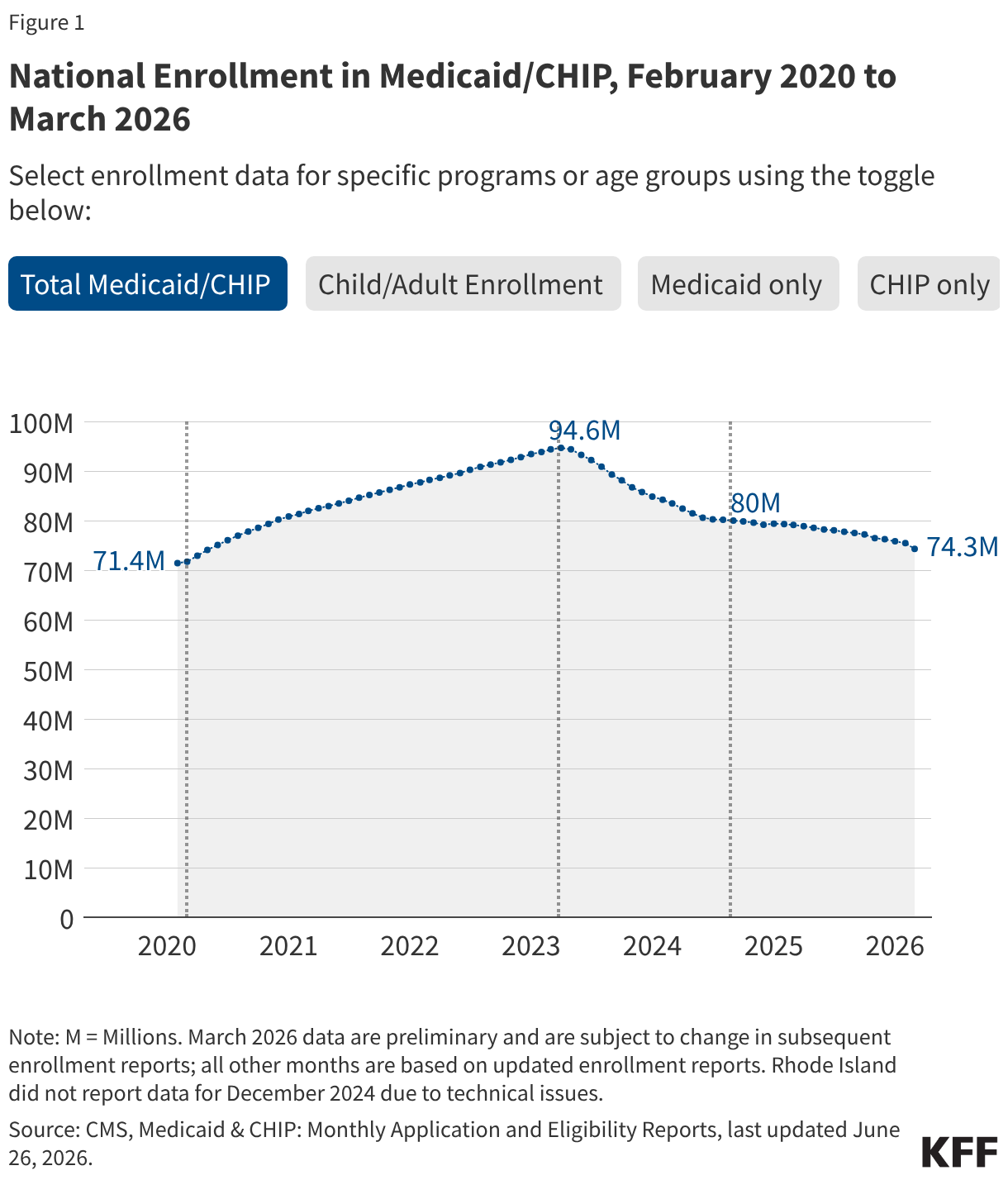
As of March 2026, national Medicaid and CHIP enrollment stands at approximately 80 million individuals. This figure is a critical marker in the program’s history, representing a significant decline from the record-breaking high of 94 million reached in March 2023.
The current enrollment data, updated monthly by the Performance Indicator Project, serves as a primary tool for tracking coverage trends. However, it is essential to note that these figures represent "full-benefit" enrollees. The data explicitly excludes individuals who receive limited benefits, such as those covered solely for family planning services. Consequently, while these figures are the gold standard for monitoring broad enrollment health, they do not constitute a census of every individual touched by the Medicaid system.
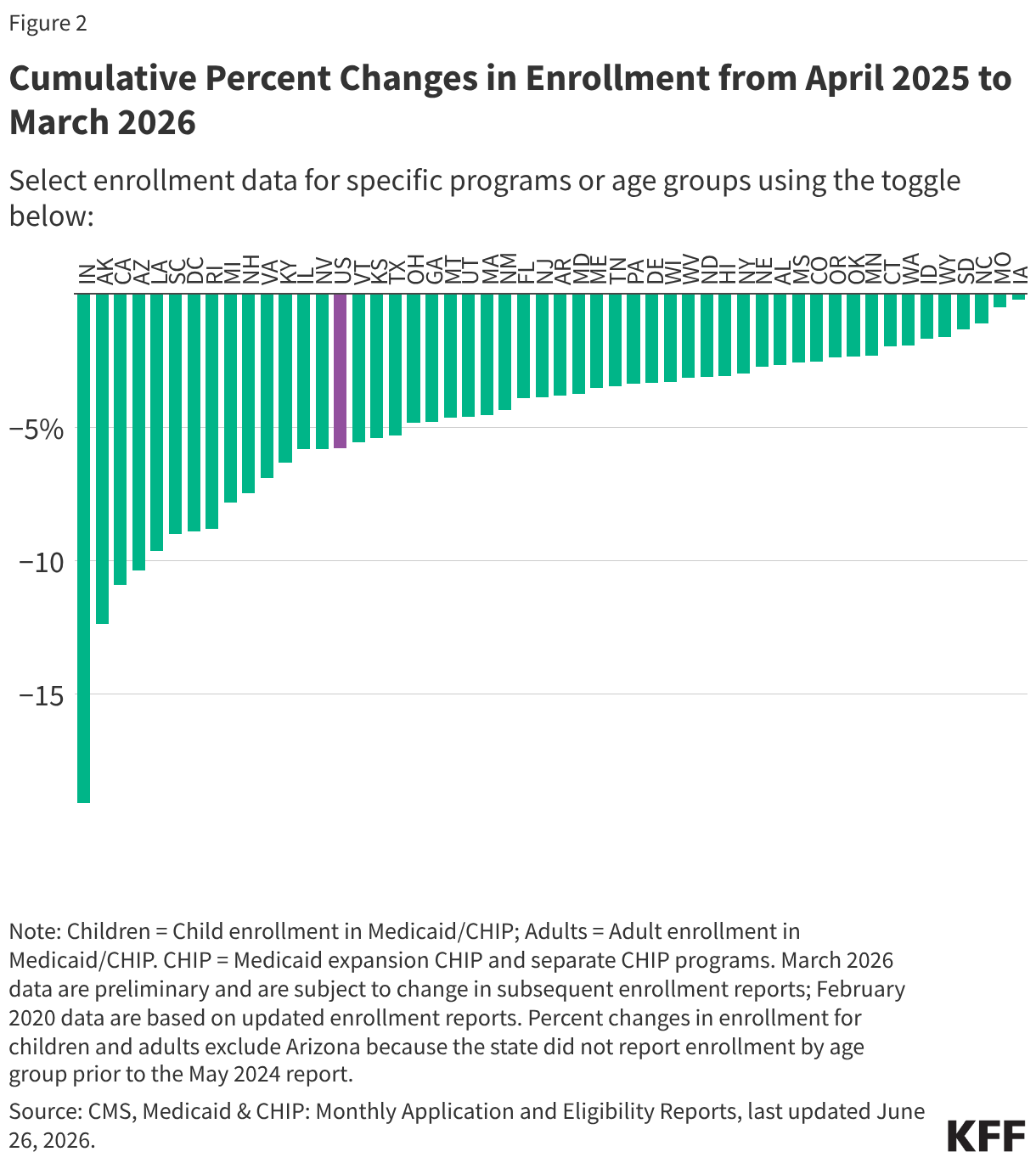
The current trends reveal a period of stabilization that was short-lived; after a brief plateau in late 2024, national numbers began a renewed decline in March 2025, a trend that experts attribute to a combination of economic factors, state-level administrative processing, and the anticipation of new federal policy mandates.
Chronology of the Medicaid Era (2014–2026)
To understand the current enrollment trajectory, one must look at the historical pivot points that have shaped the program over the last twelve years:
The Expansion Era (2014–2019)
The enactment of the Affordable Care Act (ACA) in 2014 fundamentally changed Medicaid by allowing states to extend coverage to adults with incomes up to 138% of the federal poverty level (FPL). This led to a steady increase in enrollment, peaking at approximately 75 million in March 2017. As the initial excitement of the expansion cooled, enrollment began a gradual decline, reaching 71 million by February 2020.
The Pandemic and Continuous Enrollment (2020–2023)
The onset of the COVID-19 pandemic triggered an emergency response from Congress. To ensure health security during a global crisis, federal legislation mandated that state Medicaid programs maintain continuous enrollment for participants in exchange for enhanced federal funding. This provision effectively froze disenrollments, allowing the rolls to swell to an all-time peak of 94 million by March 2023.
The Unwinding (2023–2024)
On April 1, 2023, the continuous enrollment provision expired, initiating the "unwinding" process. Over the subsequent 16 months, states began the massive administrative task of redetermining the eligibility of every enrollee. By September 2024, the impact of this process was fully realized, with total enrollment dropping to 80 million.
The 2025 Reconciliation Law (2025–Present)
The passage of the 2025 budget reconciliation bill introduced a new regulatory environment. Starting in October 2026, immigrant eligibility will be restricted, and by January 2027, strict work and reporting requirements for Medicaid expansion enrollees will go into effect, marking the most significant legislative intervention in the program’s history since the ACA.
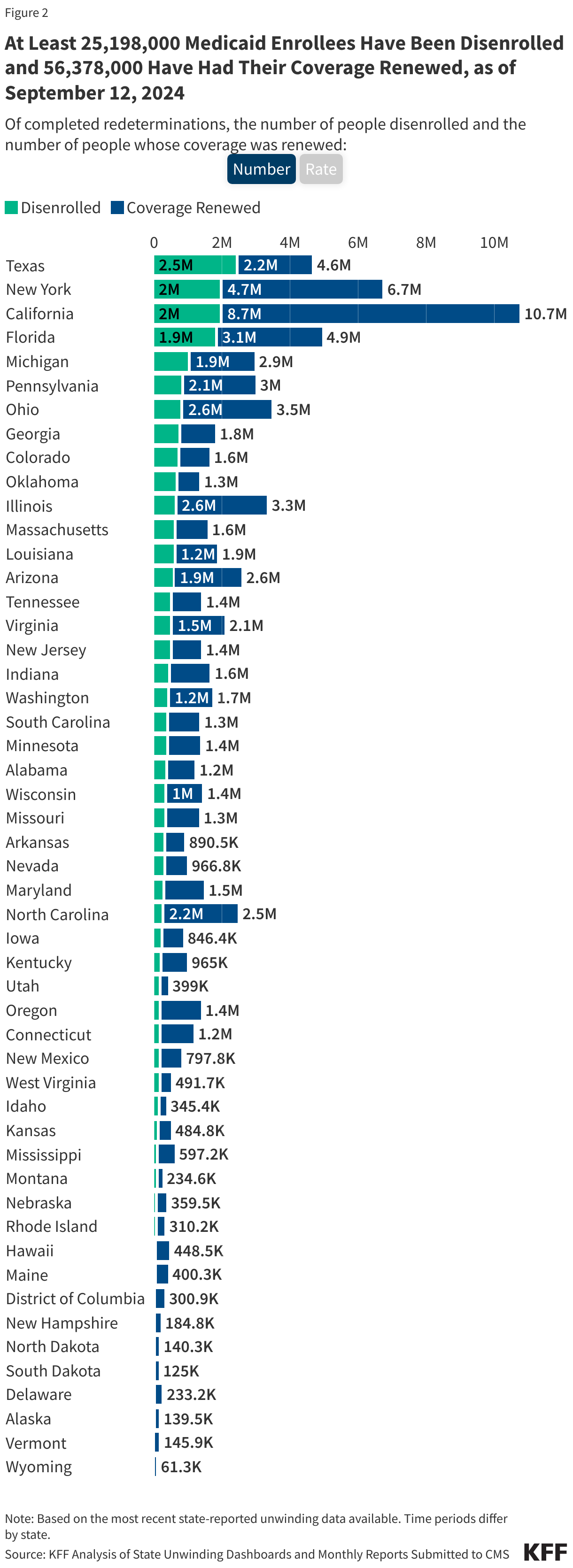
Supporting Data: The Anatomy of Disenrollment
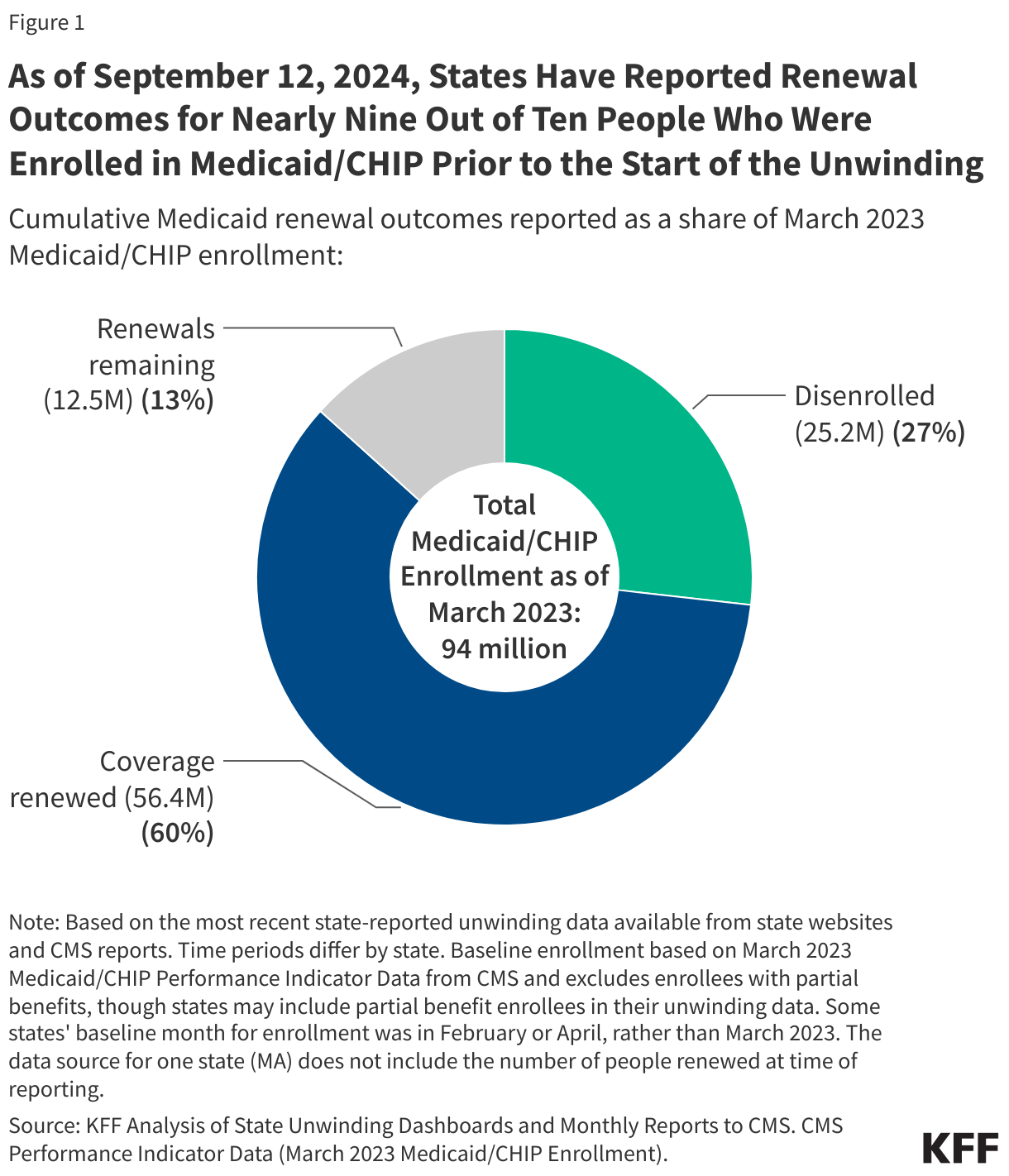
The "unwinding" process was one of the largest administrative undertakings in the history of the American social safety net. By September 12, 2024, data revealed that states had processed renewals for nearly 90% of those enrolled prior to the unwinding.
The outcomes of these renewals provide a sobering look at how coverage is lost. Of the millions of individuals who were disenrolled, a staggering 69% were terminated for "procedural reasons." Procedural disenrollment occurs when a state terminates an individual’s coverage not because they were found ineligible, but because they failed to complete the renewal paperwork, often due to missed notices, language barriers, or administrative bottlenecks.

Conversely, the data on those who successfully retained coverage highlights the success of automated systems. Approximately 61% of those who retained their coverage were renewed through "ex parte" processes—a method where the state automatically verifies eligibility using existing electronic data, requiring no action from the enrollee. This disparity between procedural termination and automated renewal highlights the importance of administrative infrastructure in maintaining health equity.
Official Responses and Policy Implications
The implementation of the 2025 reconciliation law has triggered intense debate among policymakers and health advocates. The introduction of work requirements is a cornerstone of this legislation, and it is projected to be the primary driver of enrollment declines over the next decade.
The Impact of Work Requirements
Proponents of the 2025 law argue that work requirements incentivize workforce participation and ensure that federal resources are directed toward those most in need. However, public health experts point to the "administrative burden" as a major risk. Similar to the procedural disenrollments seen during the unwinding, the complexity of reporting hours worked, navigating online portals, and providing documentation is expected to cause significant numbers of eligible individuals—particularly those in precarious employment or with limited digital literacy—to lose their coverage.
Restrictions on Immigrant Eligibility
The restriction of eligibility for certain immigrant populations, set to take effect in late 2026, represents a further tightening of the program. Analysts note that this will likely create "coverage gaps," particularly in states with high immigrant populations, potentially leading to increased uncompensated care costs for hospitals and health systems.
Long-Term Outlook
The Congressional Budget Office and various independent research entities suggest that the cumulative effect of these policies will be a sustained reduction in Medicaid enrollment relative to the status quo. For states, this means a shift in budgetary priorities. While federal funding may decrease as enrollment drops, the administrative costs associated with verifying work requirements and managing more complex eligibility checks are expected to rise, creating a new set of fiscal challenges for state-level budget planners.
Conclusion: A New Standard of Coverage
The Medicaid program is no longer the expansive, high-growth system of the pandemic years. It has entered a period of contraction characterized by rigorous eligibility scrutiny and new federal mandates. As the nation approaches the 2027 implementation of work requirements, the focus of the policy community is shifting toward the "human element" of these changes—specifically, how to ensure that the most vulnerable populations are not lost in the administrative machinery.
For observers, the data presented in this report acts as a baseline. The coming years will be defined by the tension between legislative goals of fiscal restraint and the practical realities of public health, where the loss of coverage for one individual can lead to downstream consequences for the entire healthcare system. As enrollment continues to shift, the metrics provided by CMS and the KFF trackers remain the most vital tools for understanding the health of the American safety net.
For those seeking to delve deeper into state-specific impacts or to access historical data sets, the Centers for Medicare & Medicaid Services maintains a comprehensive archive of the Performance Indicator Project. Questions regarding the methodology of these reports may be directed to specialized research entities like the Kaiser Family Foundation (KFF).