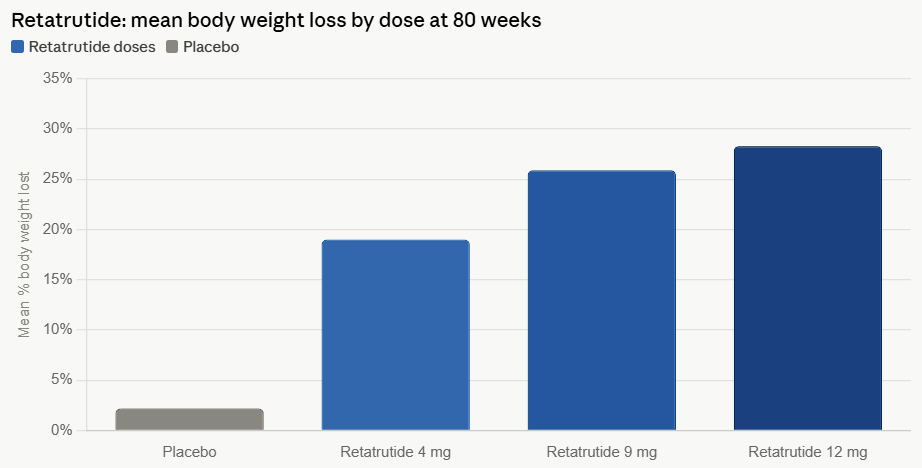
The landscape of obesity treatment is undergoing a seismic shift. Eli Lilly, already a dominant force in the cardiometabolic space with its blockbuster therapies, has pushed the boundaries of pharmacology once again. Its latest candidate, retatrutide—a triple hormone receptor agonist—has delivered unprecedented results in Phase 3 clinical trials. With an average weight loss of 28.3% over 80 weeks, the drug represents a potent new weapon against obesity. Yet, as efficacy reaches levels previously reserved for invasive bariatric surgery, the medical community is grappling with a sobering reality: the trade-off between rapid weight reduction and increasingly complex side effects.
The TRIUMPH-1 Milestone: Unprecedented Efficacy
The TRIUMPH-1 Phase 3 study has established retatrutide as a potential "gold standard" for weight loss. The triple-agonist mechanism targets three key metabolic receptors: glucagon, GLP-1, and GIP. By hitting this trifecta, the drug influences metabolism, satiety, and glucose regulation in a manner more aggressive than the current generation of dual-agonist or single-receptor therapies.
At the highest administered dose, participants experienced a staggering 28.3% reduction in body weight. To put this in clinical perspective, this result closely mirrors the weight loss outcomes observed in patients undergoing sleeve gastrectomy or gastric bypass surgery. For clinicians, this suggests that pharmacology is rapidly closing the gap between medical management and surgical intervention.
A Chronology of the Triple-Agonist Development
The development of retatrutide did not happen in a vacuum. It is the culmination of years of intense research into the incretin hormone system.
- Pre-clinical Foundations: Early research identified that while GLP-1 receptor agonists (like semaglutide) were highly effective, adding GIP and glucagon receptor agonism could amplify metabolic effects and potentially improve energy expenditure.
- Early Phase Trials: Initial human studies showed dose-dependent weight loss, with researchers noting that the titration schedule allowed for better management of gastrointestinal side effects compared to previous iterations.
- The TRIUMPH-1 Study: This pivotal Phase 3 trial was designed to test the drug across a diverse cohort of patients with obesity and varying degrees of metabolic comorbidities. The primary endpoint of 80 weeks provided a robust look at long-term sustainability.
- Present Day: Following the release of the 80-week data, the conversation has pivoted from "does it work?" to "what is the cost of such efficacy?" Regulatory bodies are now reviewing the comprehensive safety data, which includes the notable emergence of dysesthesia—a side effect that has become a major talking point in endocrinology circles.
Supporting Data: The Tolerability Gap
While the headline efficacy figures are undeniably impressive, the safety data reveals a more nuanced picture. Discontinuation rates serve as a critical proxy for patient tolerability, and at the highest dose of retatrutide, 11.3% of participants opted to stop treatment due to adverse events.
This figure is higher than the discontinuation rates reported in trials for other leading therapies:
- Tirzepatide: 6.1%
- Semaglutide: 8.0%
- Orforglipron: 10.3%
The primary culprits remain standard gastrointestinal complaints—nausea and vomiting—but the emergence of dysesthesia has added a layer of complexity. Approximately 12.5% of the high-dose group reported abnormal skin sensations, such as burning or "pins and needles." While these events were generally categorized as mild to moderate and resolved over time, their prevalence is significantly higher than in other drug trials, leading some analysts to suggest that retatrutide may be reserved for specific patient populations rather than becoming a universal first-line treatment.
Official Perspectives and Market Analysis
Industry leaders and market analysts have reacted to the data with a mixture of excitement and caution.
Kenneth Custer, executive vice president and president of Lilly Cardiometabolic Health, emphasized the strategic importance of the drug within their broader portfolio. "TRIUMPH-1 highlights the importance of options and the potential for retatrutide to help people across various stages of their obesity journey," Custer stated. He noted that the drug is designed to work in concert with existing therapies like Zepbound, allowing for a "patient-centric approach" where physicians can match the medication’s intensity to the patient’s specific needs.
Financial analysts are equally bullish but realistic. Trung Huynh of RBC Capital Markets described the trial results as a "clean win" for Lilly, citing the best-in-class efficacy. Conversely, analysts at William Blair have advised a more conservative outlook, suggesting that the tolerability profile might naturally segment the market. They predict that tirzepatide will likely remain the "go-to" medication for the general population due to its superior balance of efficacy and side-effect profile, while retatrutide may become the specialized tool for patients at the extreme end of the BMI spectrum.
The Muscle Mass and Bone Density Conundrum
One of the most pressing scientific debates currently surrounding GLP-1-based therapies is the loss of lean tissue. Rapid weight loss is rarely synonymous with fat-only loss; current data indicates that 20% to 35% of total weight reduction in these trials consists of muscle mass.
For a patient losing 70 pounds on retatrutide, this could mathematically translate to a loss of up to 24 pounds of muscle. This is not merely an aesthetic concern; muscle mass is essential for metabolic health, mobility, and structural integrity.
The Bone Density Link
The skeletal system is also under scrutiny. Research published in Nature Bone Research confirms that rapid weight loss accelerates bone resorption and decreases bone formation, leading to a decline in bone mineral density (BMD). The reduction is estimated at 1% to 3% for every 10% of body weight lost.
A 2026 presentation at the American Academy of Orthopaedic Surgeons (AAOS) meeting added weight to these concerns, noting that GLP-1 users showed a significantly higher risk of osteoporosis (4.1%) compared to matched controls (3.2%).
However, there is a silver lining in the pharmacology. Because retatrutide—and its predecessor, tirzepatide—activates the GIP receptor, there may be a compensatory protective effect. GIP receptors are present on both osteoblasts (bone-forming cells) and osteoclasts (bone-resorbing cells). Mechanistic reviews in The Journal of Clinical Endocrinology and Metabolism suggest that drugs activating the GIP receptor appear to mitigate bone density loss more effectively than those that target GLP-1 receptors alone.
Implications for Future Care
The path forward for obesity medicine is moving toward a "precision medicine" model. As the therapeutic pipeline fills with next-generation candidates—such as SciWind Bio’s XW020, which is specifically engineered to preserve muscle mass—the industry is recognizing that total weight loss is no longer the only metric of success.
Physicians must now consider a tripartite framework when prescribing these drugs:
- Metabolic Efficacy: The degree of weight loss required.
- Tolerability Profile: The patient’s ability to withstand side effects like dysesthesia or nausea.
- Tissue Preservation: The potential for long-term impact on muscle and bone health.
As the industry awaits the full publication of body composition data from the retatrutide trials, the medical community is preparing for a new era. The era of "miracle weight loss" is transitioning into an era of "managed metabolic transformation." While retatrutide stands as a testament to human ingenuity in treating obesity, it also serves as a reminder that when we manipulate the fundamental hormones of the human body, the secondary effects—both positive and challenging—require meticulous, long-term monitoring.
For the millions struggling with obesity, the arrival of such powerful tools is a beacon of hope. For the clinicians managing them, the task is to ensure that in our quest to shed the weight, we do not also shed the essential physical foundations of health.