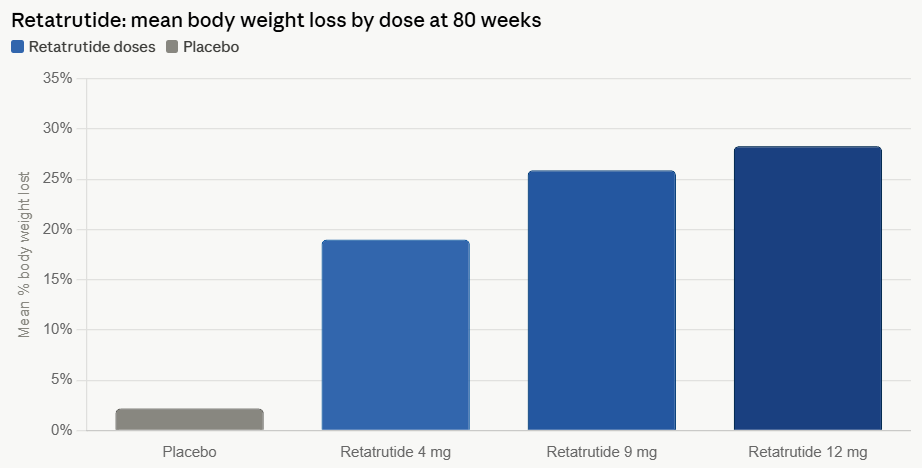
In the rapidly evolving landscape of metabolic health, Eli Lilly has reached a new, albeit complex, milestone. The pharmaceutical giant’s triple hormone receptor agonist, retatrutide, has demonstrated unprecedented weight loss efficacy in Phase 3 clinical trials, achieving an average reduction of 28.3% over an 80-week period at its highest dosage. While these results represent a potential paradigm shift in the treatment of obesity—rivaling the outcomes typically associated with bariatric surgery—they have also brought critical safety concerns to the forefront, particularly regarding muscle mass preservation, bone density, and neurological side effects.
The TRIUMPH-1 Milestone: A New Benchmark for Efficacy
The results from the TRIUMPH-1 trial underscore the transformative power of multi-receptor agonism. Unlike traditional GLP-1 agonists that target a single pathway, retatrutide stimulates the glucagon, GIP (glucose-dependent insulinotropic polypeptide), and GLP-1 receptors simultaneously.
Kenneth Custer, executive vice president and president of Lilly Cardiometabolic Health, lauded the findings, noting that the drug offers a "patient-centric approach" to obesity management. According to the data, patients on a 4 mg dose achieved nearly 20% weight loss with minimal escalation, while those on the 12 mg dose experienced transformative weight reduction. "TRIUMPH-1 highlights the importance of options and the potential for retatrutide to help people across various stages of their obesity journey," Custer stated, positioning the drug as a cornerstone of a future portfolio that includes established treatments like Zepbound and Foundayo.
Chronology of Development and Clinical Progression
The journey of retatrutide is part of a larger, aggressive push by Eli Lilly to dominate the cardiometabolic market.
- Early Development: The initial research into triple agonists was driven by the theory that targeting three metabolic pathways could address the "plateau effect" often seen with mono-agonists.
- Phase 2 Proof of Concept: Early trials established the dose-response relationship, indicating that the triple-action mechanism was safe enough to move into large-scale human testing.
- Phase 3 (TRIUMPH-1): The current trial evaluated thousands of participants over 80 weeks. The primary endpoint—significant, sustained weight loss—was met with substantial margins, outperforming the current gold standards.
- Comparative Analysis: The clinical data revealed that while efficacy is high, the "price" of this weight loss is a more challenging side-effect profile. Discontinuation rates reached 11.3% at the highest dose, notably higher than the 6.1% rate seen with tirzepatide or the 10.3% observed with orforglipron.
Supporting Data: Balancing Weight Loss and Tolerability
The data presented by Lilly paints a portrait of a powerful drug that requires careful clinical management. While the weight loss numbers are industry-leading, the profile of adverse events has drawn scrutiny from analysts.
The Dysesthesia Phenomenon
One of the most notable and unexpected side effects identified in the trial is dysesthesia—a condition characterized by abnormal skin sensations such as burning, tingling, or "pins and needles." Approximately 12.5% of participants on the highest dose reported these symptoms.
Researchers are currently investigating the mechanism behind this reaction. Hypotheses suggest that the hyper-activation of GLP-1 and glucagon receptors, which are present on peripheral nerves, may trigger these sensations. Alternatively, the rapid metabolic shift—which can deplete essential B vitamins and electrolytes—may be a contributing factor. The severity of these events is generally described as mild to moderate, with most symptoms resolving during the course of treatment, yet they remain a significant point of consideration for prescribing physicians.
The Challenge of Lean Mass Preservation
Perhaps the most significant medical challenge accompanying this level of weight loss is the reduction of lean tissue. Across the class of GLP-1 and multi-agonist medications, weight loss is rarely restricted to fat mass alone. Data suggest that 20% to 35% of total weight lost may be lean muscle mass.
For a patient losing 70.3 lbs (the average on the high-dose retatrutide regimen), this could equate to a loss of 14 to 24.6 lbs of muscle. This creates a "frailty trap": while the patient is objectively healthier due to reduced fat mass, the loss of muscle tissue can lead to decreased metabolic rate, increased risk of injury, and long-term musculoskeletal complications. Industry competitors, such as SciWind Bio, are already pivoting to develop "muscle-sparing" candidates like XW020, acknowledging that the future of weight loss is not just about the number on the scale, but the composition of the body that remains.
Official Responses and Market Implications
The financial and clinical community has reacted with a mixture of enthusiasm and caution.
Trung Huynh, an analyst at RBC Capital Markets, described the drug as a "clean win" for Lilly, citing the best-in-class efficacy. However, not all observers are as optimistic about the drug’s universal application. Analysts at William Blair have suggested that the tolerability profile of retatrutide might limit its use to patients with the highest BMIs—those for whom the risk of extreme obesity outweighs the side-effect profile. In this view, tirzepatide remains the "go-to" medication for the broader population due to its superior balance of efficacy and comfort.
Lilly’s response has been one of strategic positioning. By offering a range of treatments, they aim to tailor the medical intervention to the patient’s specific needs—a "precision medicine" approach to metabolic health.
Implications for Long-term Bone Health
The correlation between rapid weight loss and bone mineral density (BMD) decline is an emerging area of concern. A 2025 review in Nature Bone Research highlighted that for every 10% of body weight lost, patients may experience a 1% to 3% decline in BMD.
The implications are stark:
- Osteoporosis Risk: Recent data from the AAOS 2026 meeting showed that GLP-1 users faced a 4.1% risk of osteoporosis, compared to 3.2% in matched control groups.
- The GIP Protective Factor: There is a glimmer of hope in the biological mechanism of GIP. Because GIP receptors are found on bone-forming cells (osteoblasts) and bone-resorbing cells (osteoclasts), there is evidence that the GIP component of drugs like tirzepatide and potentially retatrutide may provide a protective effect, mitigating some of the expected bone loss.
Conclusion: The Path Forward
Retatrutide represents a monumental leap in the pharmacological treatment of obesity. Its ability to trigger profound, rapid weight loss is, by all metrics, a triumph of modern drug discovery. However, the path to widespread adoption is paved with the complexities of human physiology.
As clinicians move forward, the focus must shift from merely "weight loss" to "weight quality." Future guidelines will likely emphasize the necessity of concurrent resistance training and protein-rich nutrition to counteract muscle atrophy, as well as rigorous bone density monitoring. While retatrutide may soon become the most powerful tool in the physician’s arsenal, its success will depend on how effectively the medical community can mitigate its systemic side effects. As we look toward the final results of the Phase 3 trials later this year, one thing remains clear: the era of "one-size-fits-all" weight loss is ending, and the era of nuanced, patient-specific metabolic management has begun.