
For over two decades, the U.S. President’s Emergency Plan for AIDS Relief (PEPFAR) has stood as the single largest commitment by any nation to address a specific disease. Since its inception in 2003, the program has been credited with saving an estimated 26 million lives. While initially conceived as a “vertical” program—a surgical strike against the HIV/AIDS epidemic—a new, comprehensive analysis by researchers at KFF and Boston University suggests that PEPFAR’s impact has rippled far beyond the virus, serving as a critical engine for broader health system strengthening in low- and middle-income countries.
The updated findings, which extend research through 2022, demonstrate that PEPFAR’s investments in laboratory infrastructure, supply chain management, and the healthcare workforce have yielded significant "spillover" benefits, including dramatic reductions in maternal and child mortality and improved childhood vaccination rates.
Main Facts: A Broader Health Dividend
The core revelation of the study is that the success of PEPFAR cannot be measured solely by the number of antiretroviral therapy (ART) prescriptions or suppressed viral loads. By utilizing a rigorous difference-in-difference, quasi-experimental design, researchers compared health outcomes in 90 PEPFAR-supported countries against 67 low- and middle-income countries that did not receive such support.
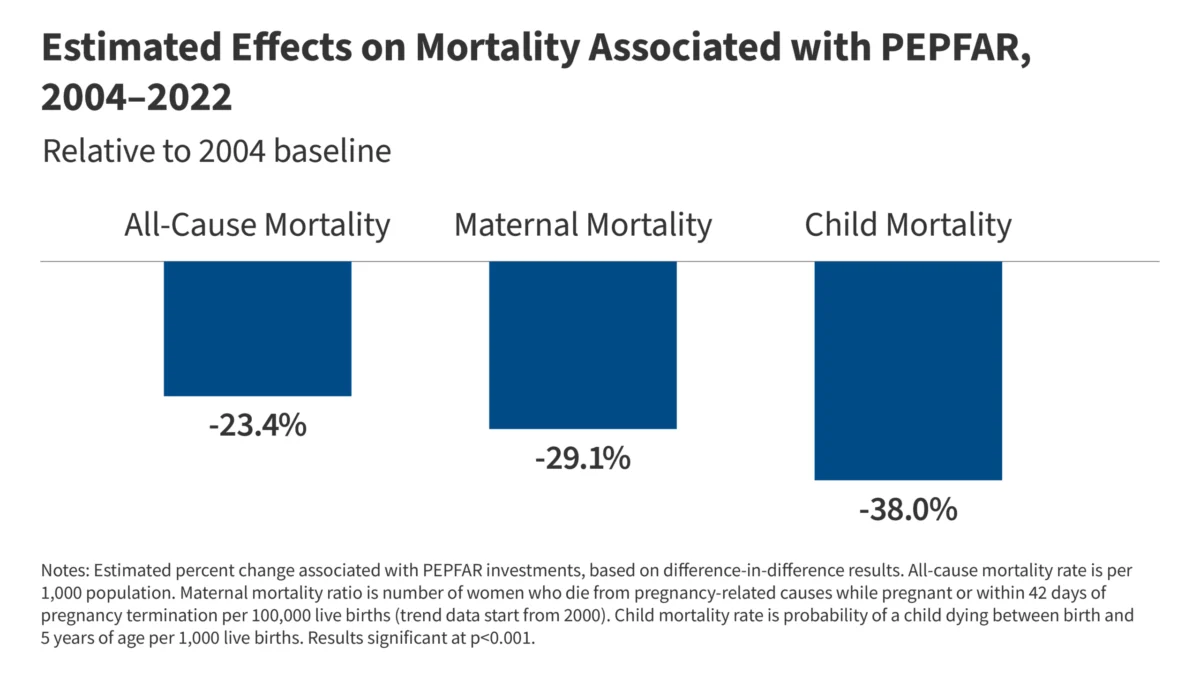
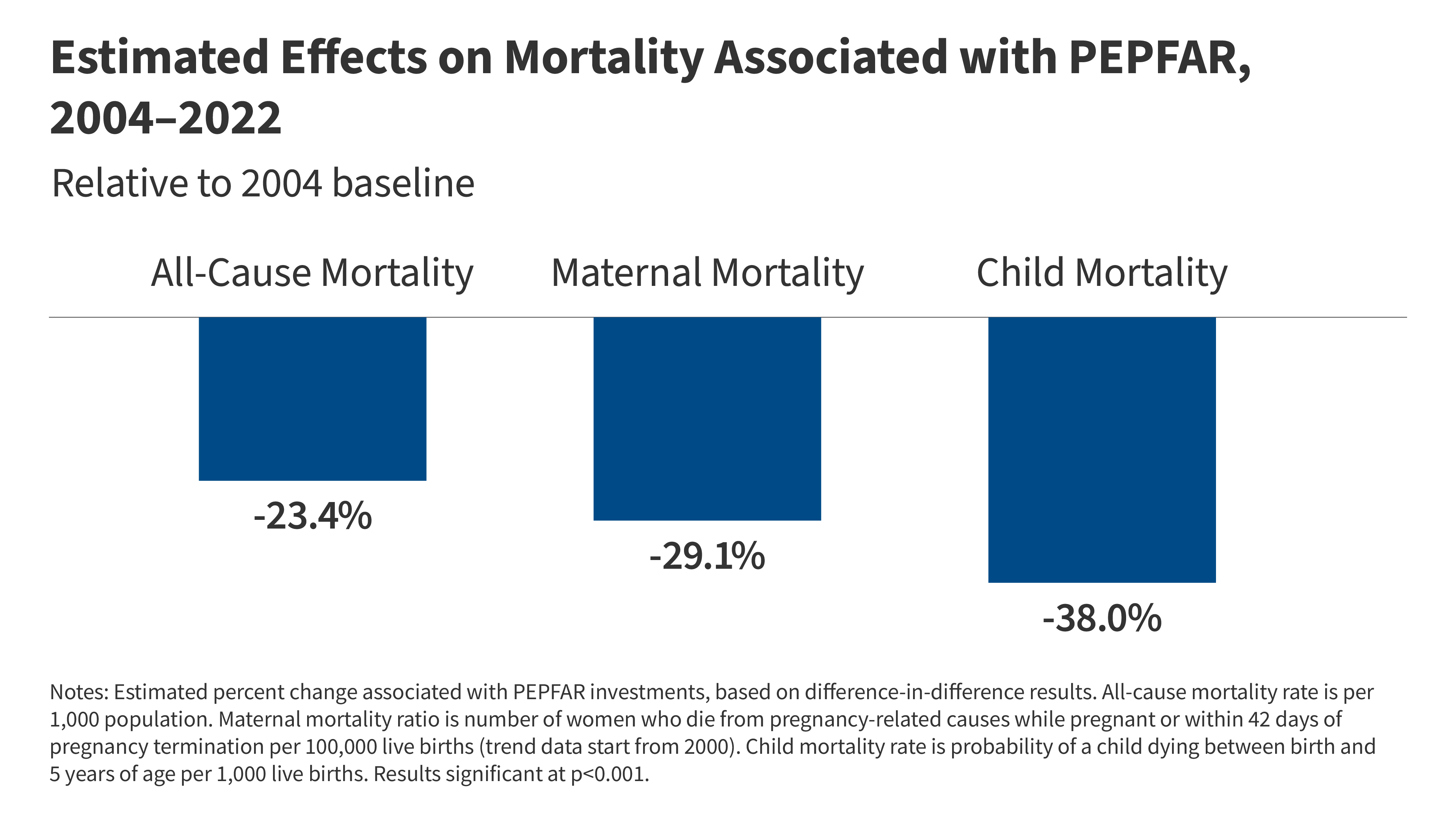
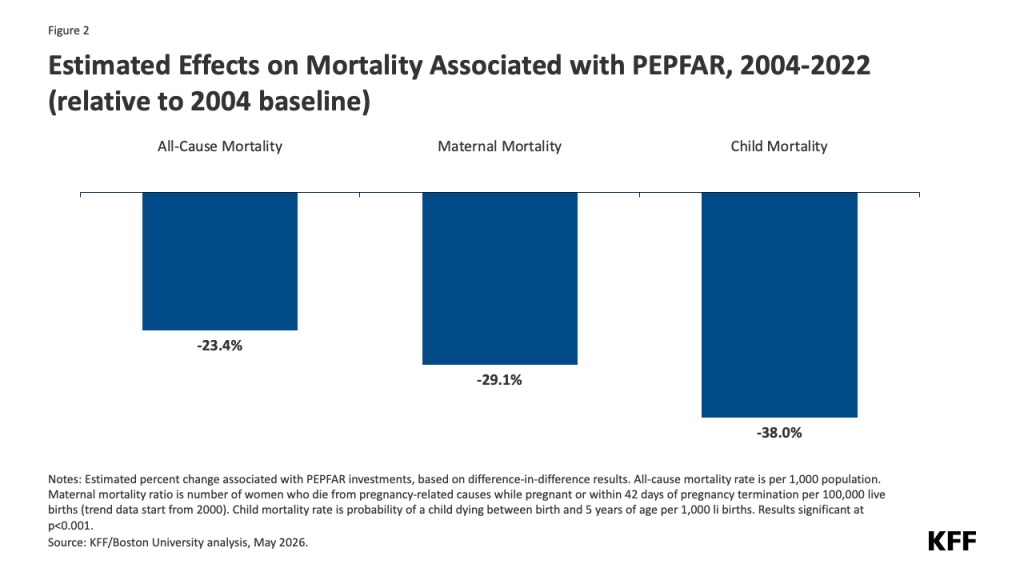
The data reveals that between 2004 and 2022, PEPFAR countries experienced statistically significant improvements in several critical health metrics:
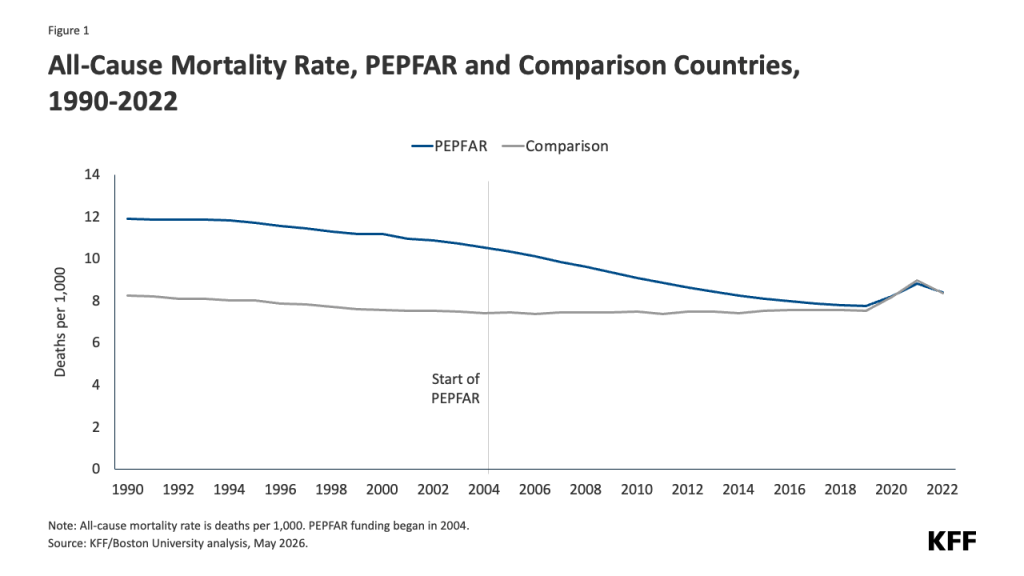
- All-Cause Mortality: A 23.4% reduction relative to the 2004 baseline.
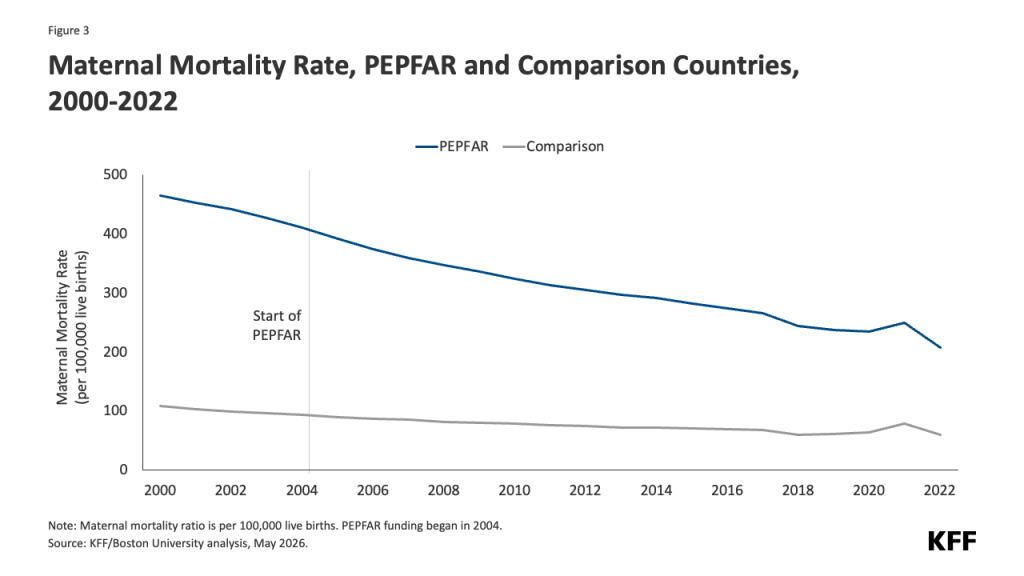
- Maternal Mortality: A 29.1% reduction in maternal mortality ratios.
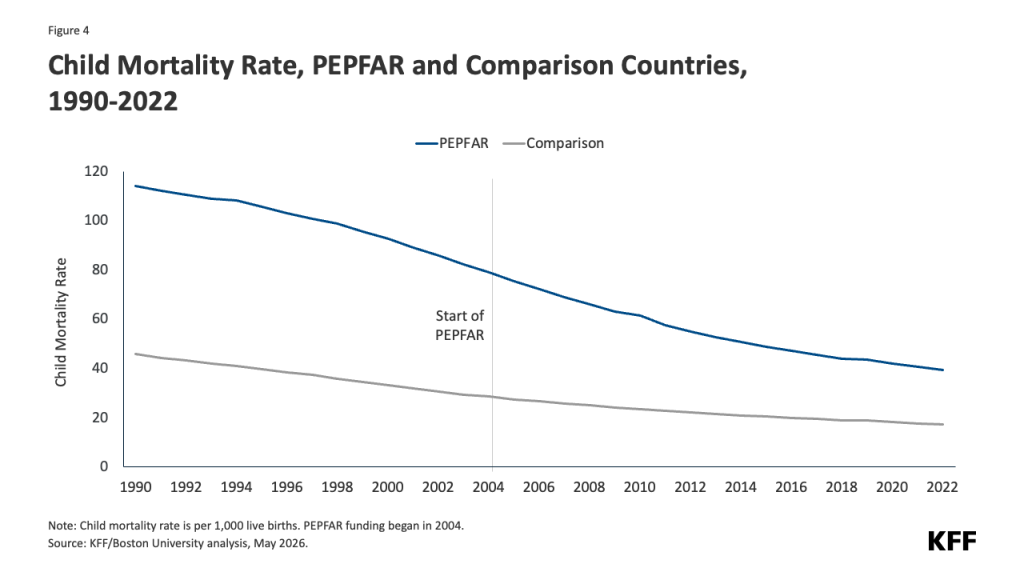
- Child Mortality: A 38.0% decrease in deaths among children under five.
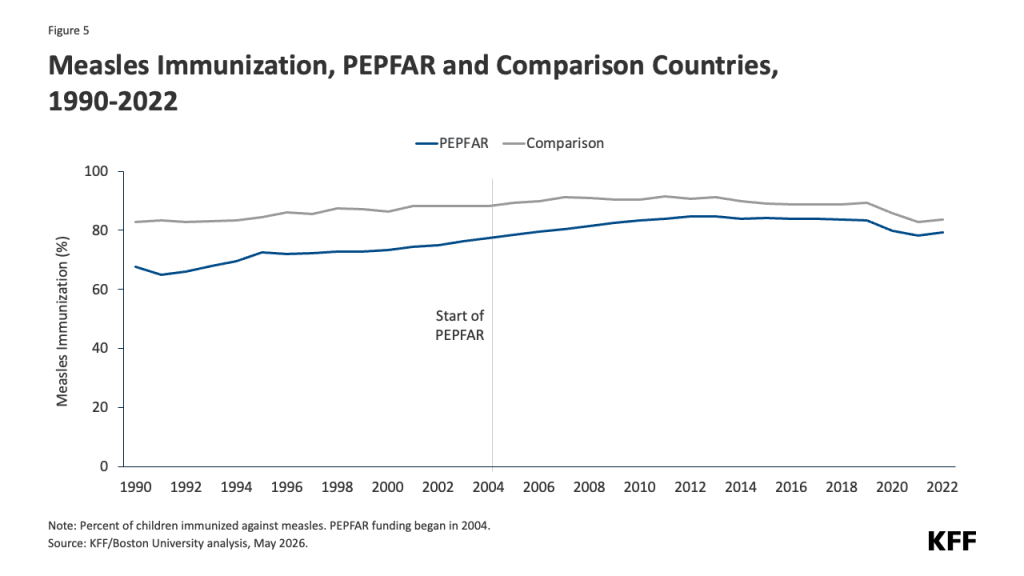
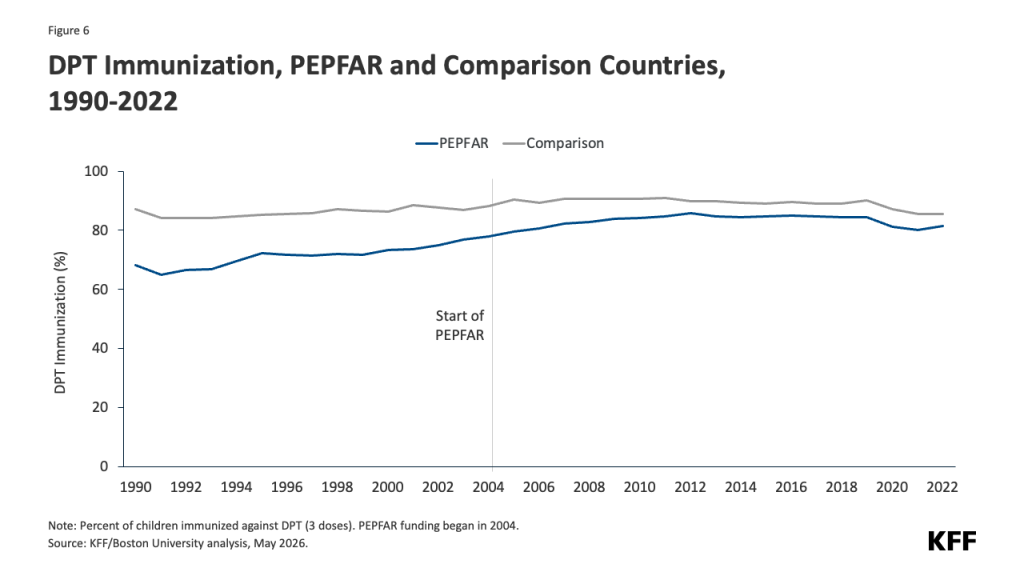
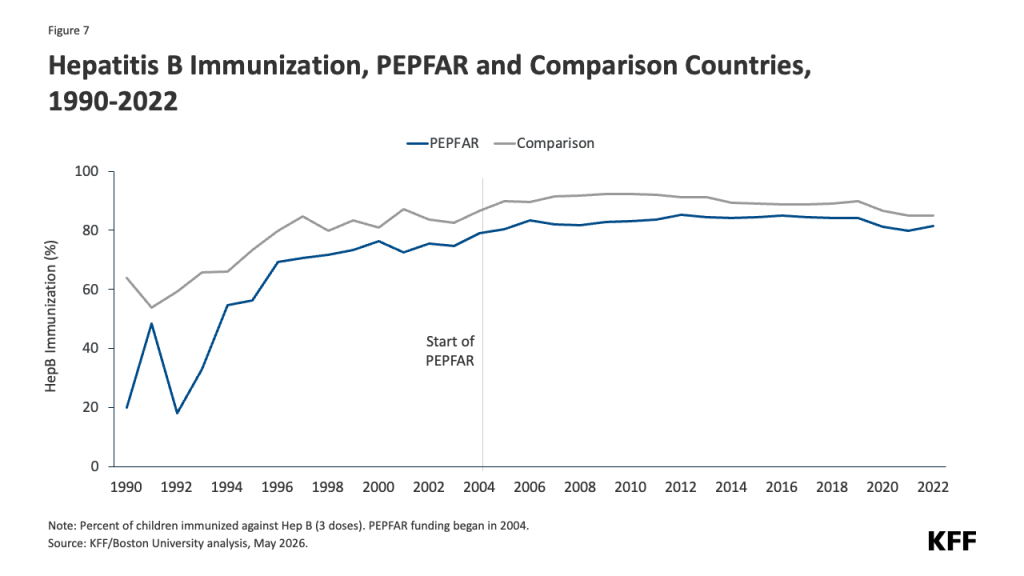
- Immunization Gains: Significant increases in coverage for measles, DPT (diphtheria, pertussis, and tetanus), hepatitis B, and protection against neonatal tetanus.
These gains occurred despite the fact that PEPFAR funding has remained relatively flat for over a decade. The results suggest that by integrating HIV services into general prenatal and primary care, PEPFAR effectively transformed from a single-disease intervention into a foundational platform for primary healthcare in many of the world’s most vulnerable regions.
A Chronology of Impact
To understand the trajectory of these health gains, it is necessary to look at the timeline of the program’s evolution:
- 2003–2004: The Launch: Initiated under the George W. Bush administration, PEPFAR arrived at a time when the HIV/AIDS pandemic was devastating the social and economic fabric of sub-Saharan Africa. The initial phase focused on rapid scaling of life-saving drugs.
- 2009–2013: Systems Integration: As the program matured, it shifted toward sustainable capacity building. Investments in laboratory diagnostics and cold-chain logistics—designed to move HIV drugs—were increasingly leveraged to support broader pediatric and maternal health services.
- 2014–2018: Resilience and Scaling: The program solidified its role as a backbone of health systems. Even as funding plateaued, the efficiency of integrated service delivery models led to continued improvements in mortality rates.
- 2019–2022: The COVID-19 Stress Test: The emergence of the COVID-19 pandemic threatened to derail two decades of progress. While the study acknowledges that the pandemic caused a global dip in health indicators, it finds that the negative impacts were universal, not isolated to PEPFAR countries. This suggests that the structural investments made by PEPFAR helped those countries remain resilient despite the unprecedented strain of the pandemic.
Supporting Data: The Evidence Base
The study’s methodology was robust, controlling for a vast array of variables including GDP per capita, population size, education, and domestic health spending. By comparing "treatment" (PEPFAR) countries with a carefully selected "control" group, researchers sought to isolate the "PEPFAR effect."
The statistical significance of these findings is striking. For instance, the reduction in child mortality (38%) is particularly notable, suggesting that the integration of HIV screening into maternal care has been a decisive factor in protecting infants. The immunization data further underscores this: while immunization rates in PEPFAR countries lagged behind the control group in the early 2000s, the gap narrowed consistently over the following 18 years.
Tables analyzed in the study highlight that even when excluding the world’s most populous nations—China and India—the results remain robust and statistically significant. This confirms that the observed health improvements are not merely statistical noise but represent a genuine, systemic improvement in the countries receiving U.S. aid.
Implications for Future Policy
The findings arrive at a precarious moment for global health diplomacy. The study explicitly notes that recent changes to the program, particularly moves to scale back funding and services, carry significant risks.
"These findings suggest that more recent changes to the PEPFAR program… could not only have negative impacts on the HIV response, but dampen improvements in other health areas," the authors conclude. The logic is clear: because PEPFAR has evolved into an integrated platform, pulling out the "HIV" thread risks unravelling the entire garment of primary care that has been woven over the last 20 years.
If the U.S. government proceeds with plans to significantly reduce the program’s footprint, the cost will likely extend beyond HIV transmission rates. It will manifest in the reversal of the hard-won gains in maternal health and the resurgence of preventable childhood diseases.
Official Responses and Expert Context
While there has been no single "official" response to this specific 2026 update, the findings align with a growing consensus among global health economists: the "silo" approach to aid is increasingly viewed as inefficient. Advocates for global health funding, such as the Kaiser Family Foundation (KFF), have long argued that PEPFAR serves as a "force multiplier."
Public health officials in partner countries have frequently cited the "PEPFAR laboratory network" as a key asset during health crises. When a new pathogen emerges, the laboratories, trained staff, and supply chain channels funded by PEPFAR often become the first line of defense. By ignoring these "spillover effects," policymakers risk underestimating the return on investment (ROI) that the U.S. taxpayer receives from global health spending.
Conclusion: The Platform Effect
The narrative of PEPFAR has always been one of extraordinary success, but for years, the debate remained trapped in a binary: is it a vertical program or a horizontal system-strengthening initiative? The data from the 2004–2022 period provides a definitive answer: it is both.
By functioning as a platform, PEPFAR has fundamentally altered the health landscape of the developing world. The 26 million lives saved from HIV are only the beginning of the story. The millions of children who survived past their fifth birthday, the mothers who survived childbirth, and the infants protected by vaccines represent a secondary, perhaps more enduring, legacy.
As Congress and the administration weigh the future of foreign aid, the evidence presented in this analysis serves as a stark reminder of the "platform effect." To dismantle the infrastructure of PEPFAR is not just to abandon the fight against HIV; it is to withdraw a vital support beam from the health systems of nations that have come to rely on that stability.
In an era of global instability and emerging health threats, the study suggests that the most prudent path is not to diminish the program, but to recognize it for what it has truly become: a bedrock of global health security that, for a relatively flat investment, continues to yield dividends that far exceed its original mandate. The challenge for the next decade will be to ensure that these gains are not only protected but expanded, ensuring that the infrastructure built to fight one disease remains a fortress against many.






