The American healthcare landscape is bracing for a fundamental shift in the administration of Medicaid. With the passage of the 2025 federal budget reconciliation law, the Medicaid program—long a safety net characterized by minimal out-of-pocket costs—is transitioning toward a model that mandates financial participation from its beneficiaries. For the first time in the program’s history, the federal government is requiring states to impose cost-sharing on adults enrolled through the Affordable Care Act (ACA) Medicaid expansion. This policy pivot, coupled with new, more stringent eligibility requirements, marks the most significant administrative overhaul of the program in over a decade.
Main Facts: A New Era of Financial Responsibility
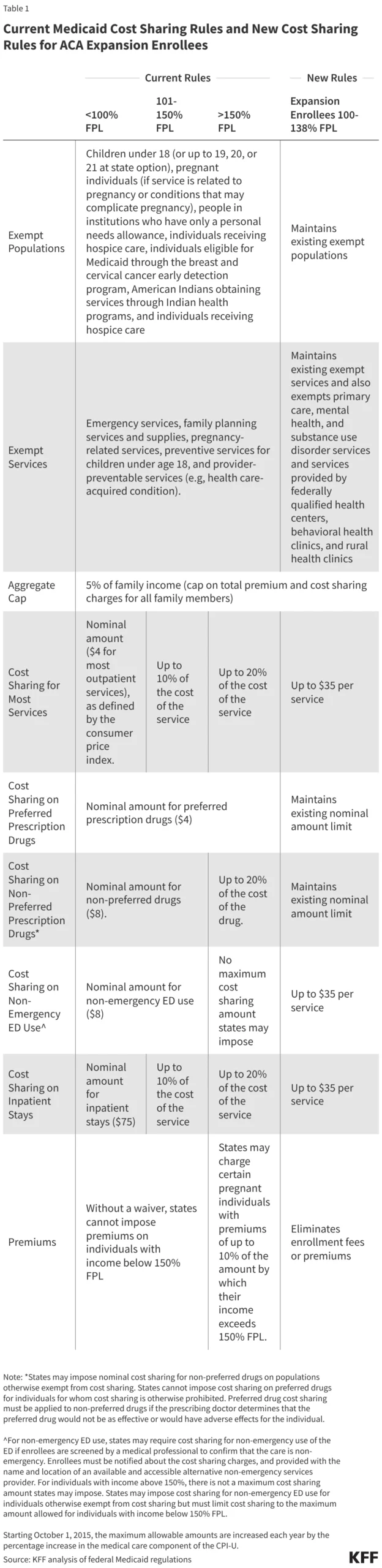
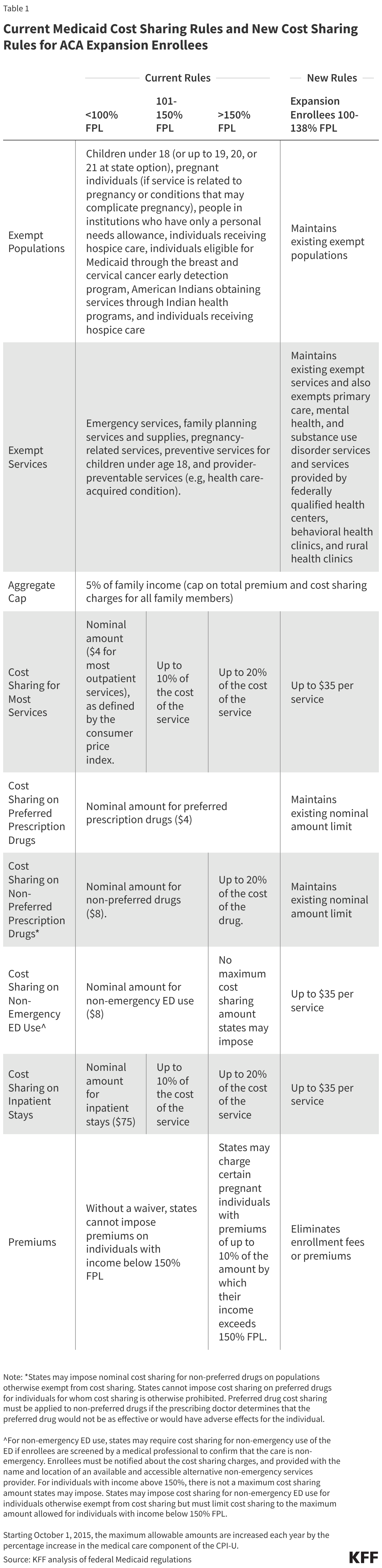
Under the new legislative framework, states are mandated to implement cost-sharing requirements for Medicaid expansion adults earning between 100% and 138% of the Federal Poverty Level (FPL). Starting October 1, 2028, these enrollees will face out-of-pocket costs of up to $35 per service.
Historically, federal rules granted states the discretion to impose nominal cost-sharing, but never the obligation. The 2025 law removes this discretionary buffer for the expansion population. While the law preserves some existing exemptions for specific services, it simultaneously introduces new administrative hurdles, including a requirement for states to conduct eligibility redeterminations every six months and the implementation of work requirements. These provisions, combined with the mandated copayments, represent a departure from the program’s founding principle of providing accessible, low-barrier care to the nation’s most vulnerable populations.
Chronology of Policy Evolution
To understand the gravity of these changes, one must look at the historical progression of Medicaid cost-sharing:
- Pre-2025 Framework: Medicaid was defined by nominal fees. While states had the option to charge for services, these were restricted to small, predictable amounts. Protections were robust: out-of-pocket costs for households were capped at 5% of income, and vulnerable populations were largely shielded from financial barriers to ensure consistent access to care.
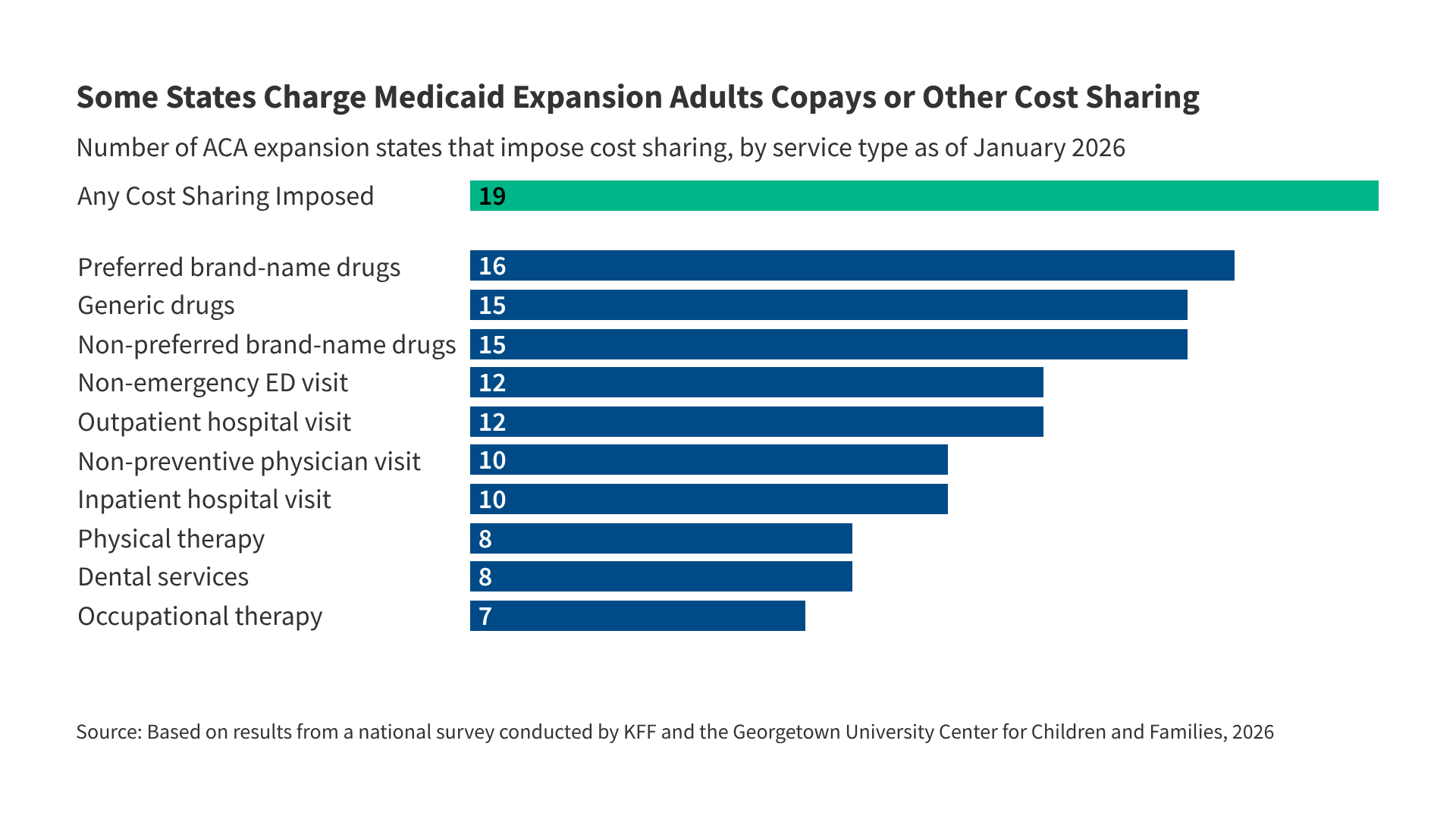
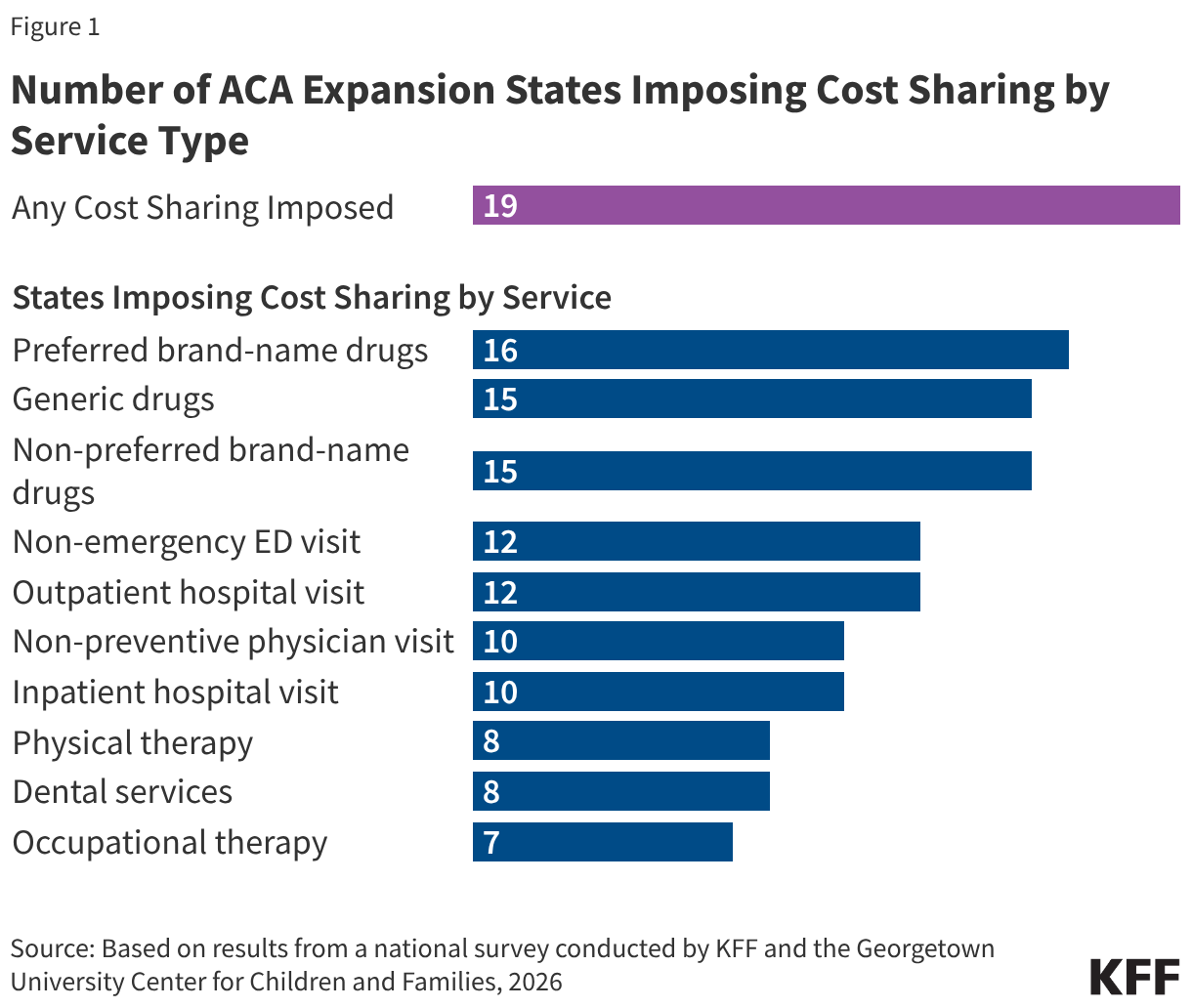
- January 2026 Status Quo: Prior to the full implementation of the 2025 law, the landscape was already fragmented. Nineteen states had independently chosen to impose some form of cost-sharing on expansion adults. The majority of these states (14) applied these fees regardless of income, while a minority targeted specific income brackets.
- The 2025 Reconciliation Law: The passage of this legislation established a federal floor for cost-sharing. It effectively standardized what was once a "state-by-state" patchwork, forcing states to align their internal policies with the new $35-per-service cap.
- October 2028 Deadline: This serves as the implementation date for the mandatory cost-sharing requirements for expansion adults (100%–138% FPL). States currently charging higher fees—such as Alaska, Michigan, Utah, and West Virginia—will be forced to reconcile their existing structures to meet the new federal mandates.
Supporting Data: The Current Landscape and Future Projections
Data collected through the 2026 Medicaid Eligibility, Enrollment, and Renewal Policies Annual Survey highlights the diverse strategies states have employed to date. Currently, prescription drugs are the most frequently targeted service for cost-sharing, with 16 states charging for preferred brand-name drugs and 15 for generic alternatives.
However, the financial burden is not uniform. In states like Alaska and West Virginia, inpatient hospital stays currently carry costs exceeding $35. These states now face the challenge of adjusting their fee schedules to comply with the federal ceiling.
Perhaps most alarming are the projections regarding individual financial impact. An analysis of Medicaid utilization patterns suggests that, if a state adopts the $35-per-service limit, an average enrollee utilizing non-exempt services could face an annual out-of-pocket burden of approximately $542. The distribution of this cost is skewed heavily toward those with the highest health needs. Older enrollees and those managing multiple chronic conditions are estimated to face costs up to five times higher than their healthier, younger counterparts.
Official Responses and State-Level Implementation
The reaction from state legislatures has been varied. Some states are proactively aligning their statutes with the new federal requirements. North Carolina, for instance, has already enacted legislation (H696) to synchronize its Medicaid copayments with the maximum levels allowable under federal law by mid-2027. This proactive stance ensures that by the 2028 federal deadline, the state will be positioned to transition seamlessly into the $35-per-service requirement.
Conversely, public health advocates and some state administrators have expressed concern regarding the administrative burden of tracking these payments. Federal law requires states to establish mechanisms to track these costs without placing the burden of documentation on the enrollee. Ensuring that these systems stop charging once the 5% household income cap is met will require significant technological investment, the cost and feasibility of which remain subjects of intense debate.
Implications: Barriers to Care and Health Outcomes
The literature surrounding Medicaid cost-sharing is extensive and points toward a consensus that is concerning to public health experts. Evidence consistently demonstrates that even nominal cost-sharing acts as a deterrent to seeking care.
The Impact on Utilization
For low-income populations, the introduction of a $35 fee is not a mere inconvenience; it is a potential barrier to essential medical services. Research indicates that when cost-sharing is introduced, utilization drops not just for "less necessary" care, but for essential services, including:
- Medication Adherence: Increased out-of-pocket costs are linked to higher rates of patients skipping doses or failing to fill prescriptions.
- Behavioral Health: Enrollees with substance use disorders (SUDs) are particularly sensitive to cost-sharing, with studies showing a direct correlation between increased fees and reduced engagement in treatment programs.
- Preventative Screenings: Necessary screenings for cancer and other chronic diseases are often deferred when costs are perceived as prohibitive.
Long-term Health Consequences
The clinical implications are dire. Studies observing older and low-income populations suggest that the introduction of financial barriers to care is associated with higher mortality rates. Because Medicaid expansion enrollees often suffer from a higher prevalence of chronic physical and behavioral health conditions compared to the general population, the impact of these new requirements will likely be disproportionately felt.
The "vicious cycle" created by these policies is clear: by increasing the cost of managing chronic conditions, the state may inadvertently reduce the number of people who successfully manage their health. This leads to an increase in high-cost emergency room visits—the very outcome that many state policies claim to reduce—as patients wait until their conditions reach a crisis point before seeking help.
Conclusion: A Delicate Balance
The 2025 reconciliation law represents a fundamental ideological shift in how the United States views the Medicaid program. By moving away from a model of near-universal, no-cost access for the lowest-income individuals, the government is attempting to curb program spending and enforce a sense of "individual responsibility."
However, the empirical evidence suggests that the cost of these savings may be paid in the health of the enrollees. As states prepare for the October 2028 implementation, the focus must shift to how they will protect the most vulnerable from being priced out of their own care. The success of this policy will not be measured by the revenue collected from copayments, but by whether or not it maintains the accessibility that has defined the Medicaid program for over half a century.
Policymakers and stakeholders must continue to monitor the impact of these changes closely, utilizing annual survey data and claims analysis to ensure that the "protection" of the Medicaid budget does not come at the expense of the patients it was created to serve.