
Introduction: A New Global Health Crucible
The Democratic Republic of the Congo (DRC) is currently grappling with a severe and rapidly escalating Ebola outbreak that threatens to destabilize the Great Lakes region of Africa. First detected on May 15, 2026, the outbreak has moved with alarming speed, crossing international borders into Uganda and prompting the World Health Organization (WHO) to designate it a "Public Health Emergency of International Concern" (PHEIC).
This crisis arrives at a precarious moment in the history of international development. As global health systems continue to recover from previous pandemics and navigate shifting fiscal priorities, this outbreak serves as the first major "stress test" for the current U.S. administration’s revised approach to foreign assistance. With nearly 746 suspected cases and over 176 deaths reported as of May 21, the international community is scrambling to determine whether existing cooperative frameworks are sufficient to contain a pathogen that has historically proven both lethal and elusive.
The Chronology of the Crisis
The rapid trajectory of this outbreak has left health authorities little room for error. The following timeline outlines the acceleration of the crisis:
- May 15, 2026: Initial reports emerge of a cluster of hemorrhagic fever cases in northeastern DRC. Local health authorities alert regional WHO offices, triggering early investigation protocols.
- May 17, 2026: After confirming the presence of the Ebola virus and noting the first cross-border transmission into Uganda, the WHO Director-General officially declares a PHEIC. This designation signals to donor nations that the crisis requires immediate, coordinated global intervention.
- May 19, 2026: Epidemiological modeling suggests the outbreak is spreading faster than initial estimates, exacerbated by the mobility of populations in the Ituri province and the porous nature of the DRC-Uganda border.
- May 21, 2026: Official counts reach 746 suspected cases and 176 suspected deaths.
- May 23, 2026: This policy review is updated to reflect that, while containment efforts are underway, the viral strain involved—the Bundibugyo strain—presents unique challenges, including the historical scarcity of available vaccines compared to the Zaire strain often seen in previous outbreaks.
Epidemiological Landscape and Historical Context
The current outbreak is not occurring in a vacuum. The DRC has faced numerous Ebola outbreaks since the virus was first discovered in 1976. However, the experience gained during the 2014-2015 West African epidemic and the 2018-2020 DRC outbreaks is now being tested against a different set of geopolitical and logistical variables.
The Complexity of the Bundibugyo Strain
Unlike the Zaire Ebolavirus, which has seen significant vaccine development, the Bundibugyo strain presents a more complex landscape. Because it is less frequent, the pharmaceutical pipeline for countermeasures is not as robust. This forces health organizations to rely heavily on traditional containment strategies: contact tracing, the establishment of Ebola Treatment Units (ETUs), and rigorous infection prevention and control (IPC) measures in hospitals.
Logistical and Social Hurdles
The region remains plagued by infrastructure limitations and intermittent insecurity, which complicates the movement of medical supplies and the deployment of personnel. Furthermore, public trust—a cornerstone of successful containment—is fragile. In many communities, skepticism toward international intervention remains a significant barrier to effective community engagement and vaccination uptake.
The Multi-Layered Response: Official Actions
The international response is characterized by a "cluster" approach, where local, regional, and international actors operate in tandem.
WHO and Regional Coordination
The World Health Organization is currently acting as the central nervous system for the response, coordinating with the Africa CDC to harmonize surveillance data across the DRC-Uganda border. Their primary mandate is to prevent the spillover into urban centers, where population density could turn a regional outbreak into a catastrophic urban epidemic.
The NGO Ecosystem
Organizations such as Médecins Sans Frontières (MSF), the International Rescue Committee (IRC), and CARE International are on the front lines, setting up isolation centers and providing psychosocial support to families affected by the virus. These organizations are essential for bridging the gap between national government directives and local community realities.
U.S. Global Health Policy: A New Paradigm
The United States has historically been the primary financier of global health security. However, this outbreak is unfolding under a new fiscal and policy framework established by the Trump administration.
Shifts in Operational Mechanisms
The U.S. government has initiated its response, but the mechanisms of support are distinct from previous iterations. There has been a notable move toward decentralized funding and an emphasis on "America First" priorities within the global health budget. This has led to:
- Reduced Centralized Oversight: A shift away from large-scale, long-term multinational programs toward more targeted, bilateral agreements.
- Fiscal Constraints: The current budgetary environment has placed a premium on proving the "return on investment" for global health spending, forcing agencies like USAID and the CDC to justify every dollar in a highly competitive fiscal climate.
- Strategic Realignment: The U.S. is prioritizing the protection of its own borders and the minimization of domestic risk, which, while pragmatic, complicates the altruistic diplomacy that historically defined U.S. global health efforts.
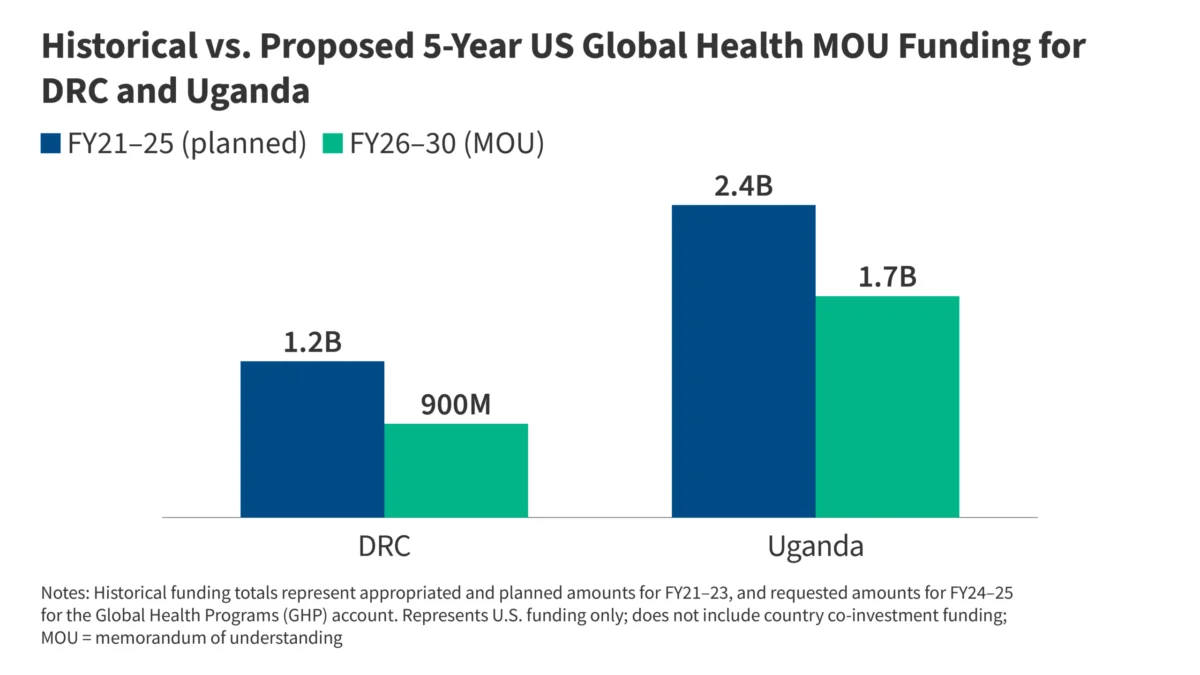
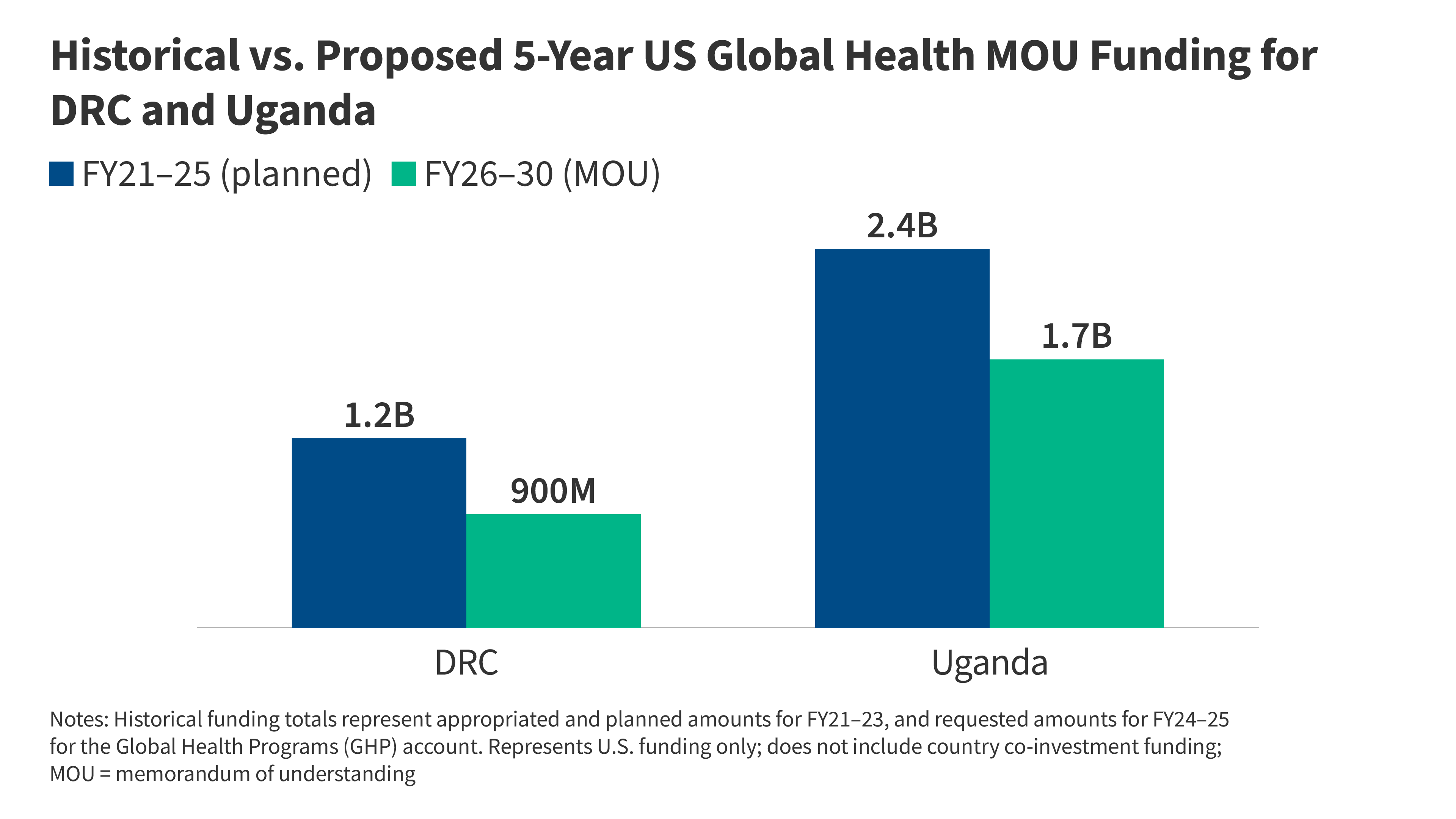
The Data Gap
As shown in recent policy briefings, the proposed five-year funding projections for DRC and Uganda indicate a cooling of U.S. financial commitment. Whether this is a temporary realignment or a permanent shift in strategy remains the subject of intense debate in Washington.
Implications: The Great Test
This Ebola crisis represents more than just a medical emergency; it is a test case for the resilience of the global health architecture.
Questioning U.S. Commitment
The most pressing question for policymakers is whether the current U.S. infrastructure can scale effectively in an emergency. If the U.S. response remains constrained by the new administrative barriers, the resulting vacuum in leadership may be filled by other international actors, or worse, left unfilled.
The Future of Global Health Security
The international community must address several key questions as the outbreak continues:
- Sustainability: Can the current response be sustained if the outbreak lasts for months rather than weeks?
- Surveillance: Is the cross-border data-sharing mechanism sufficiently transparent to detect further spread into neighboring countries like Rwanda or South Sudan?
- Governance: Does the current international response system have the authority to bypass bureaucratic hurdles that have historically slowed the deployment of emergency aid?
Conclusion: Lessons for an Uncertain Future
The Ebola outbreak in the DRC and Uganda is a stark reminder that the era of "easy" containment is over. The convergence of regional instability, the emergence of a difficult-to-treat viral strain, and the reconfiguration of U.S. global health policy creates a perfect storm.
For the U.S., this is the "hantavirus of international policy"—a moment that will either demonstrate the efficacy of a more fiscally conservative, decentralized global health strategy or expose its fundamental weaknesses. As the international community monitors the situation, the focus must remain on rapid, evidence-based intervention. History has shown that in the face of an Ebola outbreak, hesitation is the greatest ally of the virus. Only through sustained coordination, transparent data sharing, and a robust commitment of resources—regardless of the political climate—can the world hope to contain this escalating threat.
The next few months will be critical. If the response succeeds, it may provide a template for future outbreaks; if it falters, it may signal the end of a decades-long commitment to global health security that has saved millions of lives. The eyes of the world are now firmly fixed on the border regions of the DRC, waiting to see if humanity can rise to meet this latest, most complicated test.






