In the modern digital economy, the promise of Artificial Intelligence is often framed as a catalyst for efficiency, innovation, and democratization. Yet, in the case of Medvi, a telehealth entity currently projected by its founder to reach a $1.8 billion valuation, AI has served a different purpose: it has become the engine for a sophisticated, high-speed customer acquisition machine that operates within the shadows of federal oversight.
While recent profiles in mainstream media have lauded Medvi as a testament to the "one-person company" era, a more critical investigation reveals a landscape of misbranded pharmaceuticals, AI-generated fabrications, and a business model meticulously engineered to evade the jurisdictional reach of the FDA, the FTC, and state medical boards.
The Anatomy of an Outsourced Empire
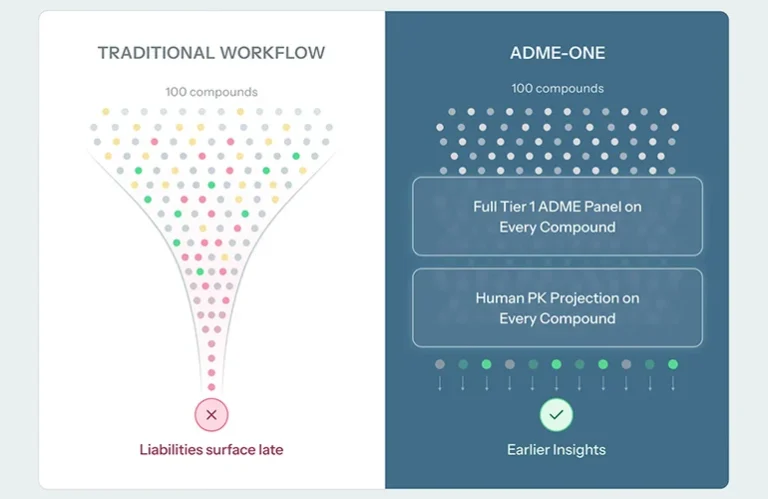
Medvi’s business model is a masterclass in regulatory arbitrage. Unlike a traditional pharmacy or medical clinic, Medvi does not own a single facility, nor does it employ a single physician. Instead, it functions as a high-volume marketing layer that sits atop an ecosystem of third-party vendors.
By outsourcing the clinical and pharmaceutical components of its operation to firms like CareValidate, OpenLoop Health, Beluga Health, and Belmar Pharma Solutions, Medvi has effectively offloaded the legal burden of healthcare delivery. When a patient clicks on a Medvi advertisement, they are not entering a medical practice; they are entering a data-collection funnel. The prescribing is performed by clinicians contracted through third-party platforms, and the medication is dispensed by external compounding pharmacies. This structural design ensures that if a patient is harmed, or if a prescription is deemed inappropriate, the liability is fragmented across a web of contractors, leaving Medvi—the entity generating the demand—largely shielded from the consequences.
A Chronology of Compliance and Controversy
The trajectory of Medvi’s ascent is punctuated by red flags that have, to date, failed to curb its growth.
- May 2025: An investigative report by Futurism exposes widespread use of AI-generated content on Medvi’s platform. The report highlights fabricated patient testimonials, doctored "before-and-after" photos, and fake doctor endorsements designed to manufacture social proof.
- February 2025: The FDA formally declares the national shortage of semaglutide resolved. This declaration effectively terminates the "compounding loophole" that had allowed telehealth firms to bypass standard FDA approval processes by selling unauthorized copies of branded drugs like Ozempic and Wegovy.
- February 2026: The FDA issues a formal warning letter to Medvi, citing the company for severe misbranding violations. The agency explicitly notes that Medvi’s marketing materials falsely implied the company was a drug manufacturer and suggested that its compounded products possessed FDA approval—a direct violation of the Federal Food, Drug, and Cosmetic Act.
- April 2026: Despite the warning letter and the closure of the compounding loophole, Medvi continues to project a $1.8 billion valuation, fueled by its aggressive customer acquisition tactics and the continued distribution of metabolic drugs.
The Compounding Crisis: High Risk, Low Oversight
The proliferation of compounded GLP-1 drugs represents one of the most significant public health risks in the current telehealth landscape. When the FDA initially declared a shortage of semaglutide in 2022, it provided a narrow window for pharmacies to produce copies to meet patient needs. However, companies like Medvi moved rapidly to monetize this window, creating a massive, unregulated marketplace.
The danger of these compounds is not theoretical. Independent analysis conducted by Novo Nordisk—the manufacturer of Ozempic and Wegovy—found that some injectable semaglutide products sourced from compounding pharmacies contained up to 86% impurities. Despite these findings and the official resolution of the shortage, the industry has proven remarkably resilient. When Hims & Hers, another major player in the space, attempted to continue selling compounded versions of Novo Nordisk’s newly approved Wegovy pill, it triggered a patent infringement lawsuit. While that specific litigation concluded in a distribution agreement, it underscored the desperation of telehealth firms to maintain access to high-margin, off-label metabolic drugs.
The Tripartite Regulatory Failure
The Medvi case exposes a systemic collapse in inter-agency coordination. The healthcare infrastructure used by companies like Medvi is governed by three distinct federal entities, each operating within its own silo:
- The FDA: Responsible for the drug itself, the legality of the compounding, and the accuracy of the labeling. While the FDA issued a warning letter to Medvi, it characterizes such letters as "informal and advisory," providing little immediate deterrent to a company scaling at breakneck speed.
- The FTC: Charged with policing unfair and deceptive advertising practices. The FTC has the authority to prosecute the kind of AI-generated fraud documented by Futurism. However, the agency’s investigative process is notoriously slow, often taking years to reach a consent decree—by which time a company like Medvi may have already realized its exit strategy or served thousands of unsuspecting patients.
- State Medical Boards: Responsible for the standard of care. These boards are designed to evaluate the conduct of individual physicians, not the algorithmic infrastructure that facilitates thousands of asynchronous clinical encounters. When a patient in New York is prescribed a drug by a doctor in Texas via a platform run in Delaware, the jurisdictional ambiguity creates a "regulatory no-man’s-land."
The Telehealth "Asynchronous" Problem
At the heart of the Medvi model is the rise of "asynchronous prescribing." In traditional medicine, a patient-physician relationship is built upon a synchronous, often in-person or live video encounter. In the Medvi model, the "consultation" is often little more than a digitized intake form.
State medical boards remain divided on whether these automated questionnaires satisfy the legal requirements for establishing a valid medical relationship. While some states mandate live video visits for high-risk medications, others have weaker standards. Medvi’s ability to operate in 49 states allows it to pivot based on the path of least resistance, exploiting the lack of a unified national standard for telehealth practice. Because Medvi outsources this function to companies like OpenLoop Health, it maintains a convenient layer of deniability: if a standard of care is breached, the blame is placed on the clinician, not the company that designed the automated flow.
Implications for the Future of Digital Health
The Medvi saga is not an anomaly; it is a symptom of a broader shift in the healthcare industry. We are witnessing the end of an era where drug manufacturing, clinical prescribing, and marketing were siloed, regulated industries. Today, these functions have been collapsed into a single digital user experience.
The current regulatory framework, which relies on reactive enforcement and agency-specific mandates, is fundamentally ill-equipped to manage this convergence. The FDA cannot regulate the advertising, the FTC cannot regulate the practice of medicine, and state medical boards cannot regulate the technology infrastructure.
To prevent further exploitation of these gaps, the industry requires a significant legislative intervention. This includes:
- Platform Liability: Creating a legal framework that holds digital health platforms accountable for the clinical outcomes and advertising claims of the vendors they host.
- Coordinated Oversight: Establishing a cross-agency task force—comprising the FDA, FTC, and representatives from state medical boards—to monitor and audit high-growth telehealth firms in real-time.
- Standardized Telehealth Requirements: A federal baseline for what constitutes a valid clinical encounter for high-risk medications, superseding the current patchwork of state regulations.
Until such measures are enacted, the gap between innovation and regulation will continue to widen. Medvi’s $1.8 billion projection is a testament to how profitable that gap has become. For the patient, however, the price of this "efficiency" may be far higher than the cost of a monthly subscription. As the industry continues to leverage AI to maximize patient acquisition, the lack of a robust, unified regulatory response ensures that the next billion-dollar company will be built on the same shaky foundation of outsourced accountability and questionable marketing.