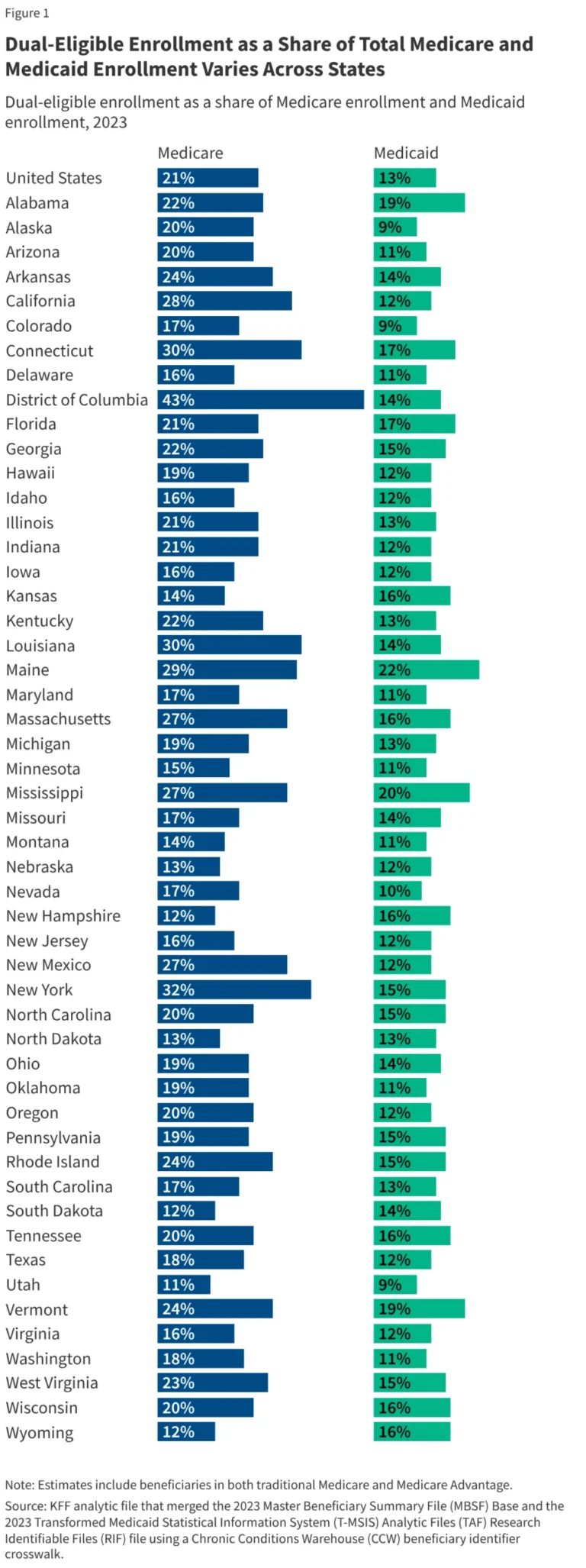
Medicaid serves as a critical lifeline for millions of Americans, covering roughly one-fifth of all adults living with substance use disorders (SUDs). For those facing the most severe symptoms, inpatient and residential treatment—often referred to as the "highest levels of care"—are essential components of the recovery continuum defined by the American Society of Addiction Medicine (ASAM).
However, for decades, a federal policy known as the "IMD payment exclusion" has restricted Medicaid from paying for services provided in Institutions for Mental Disease (IMDs)—facilities with more than 16 beds primarily focused on mental health or substance use treatment. This longstanding barrier left a massive gap in the safety net, forcing states to shoulder the burden of residential care alone.
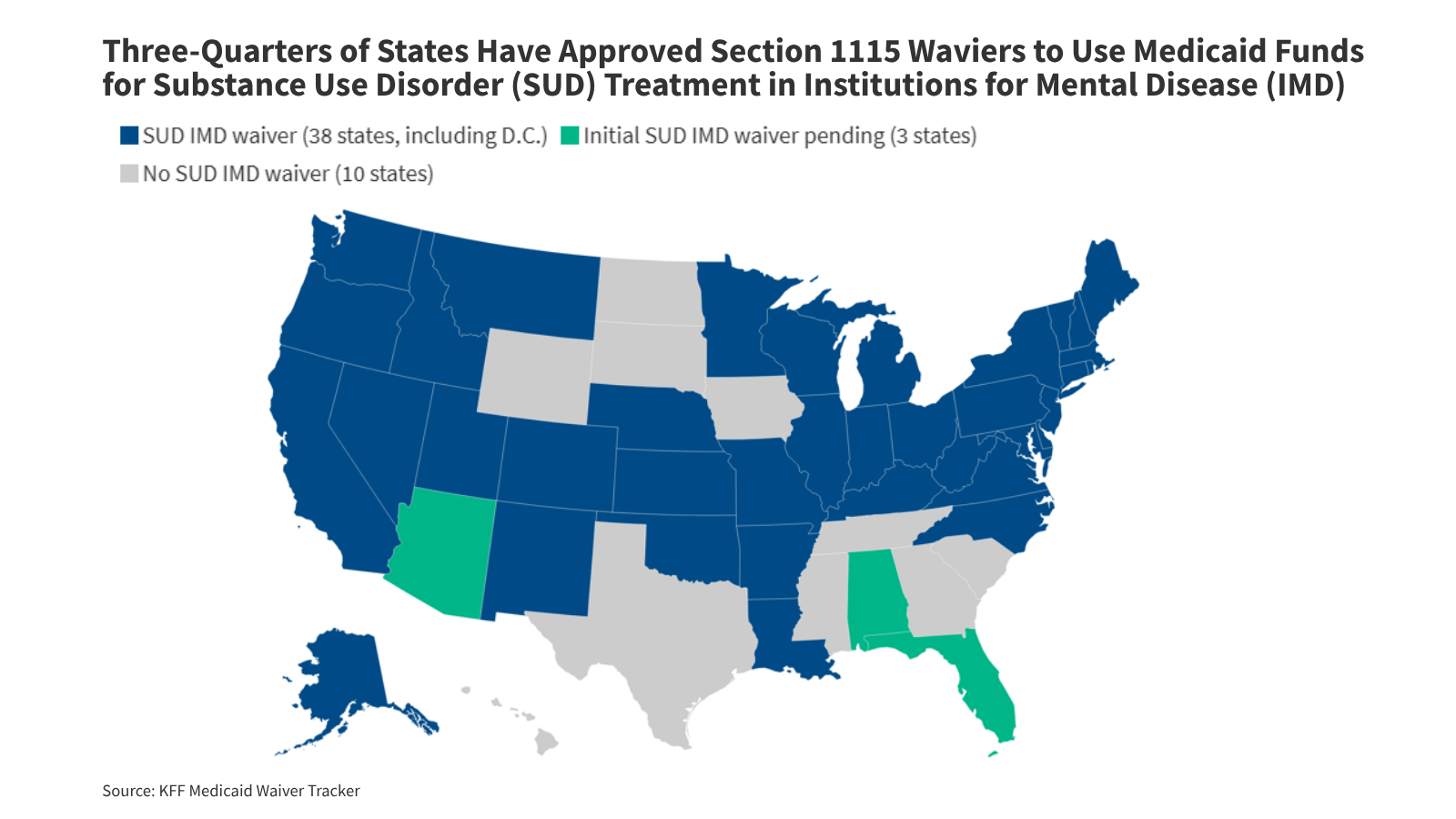
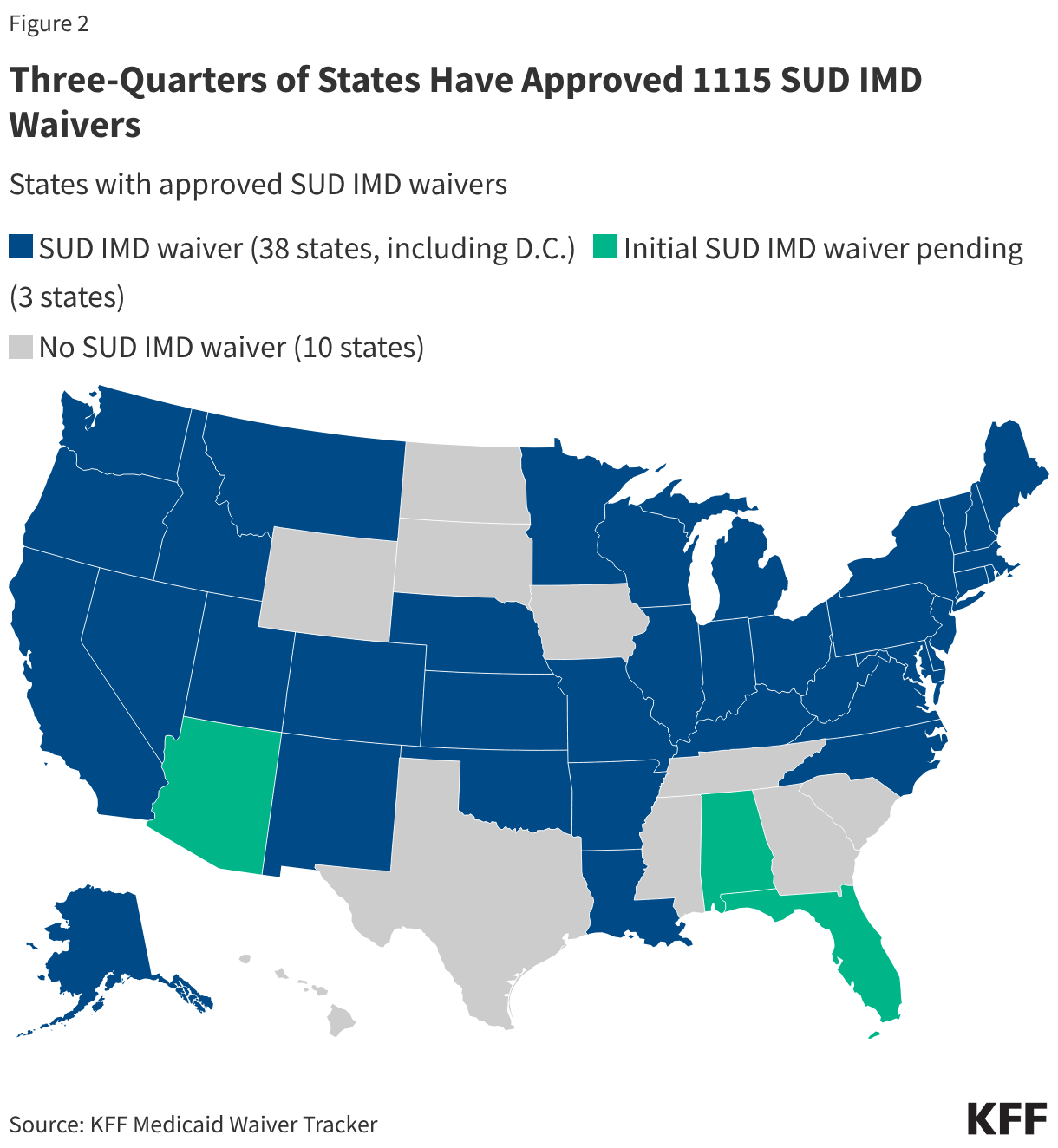
Today, that landscape is shifting. Through Section 1115 demonstration waivers, 38 states have now been granted authority to bypass this exclusion, allowing them to use federal Medicaid funds to treat SUDs in larger residential and inpatient settings. As the first wave of these waivers completes its evaluation cycle, a complex picture emerges: while access to care has undeniably expanded, the challenges of workforce shortages, administrative friction, and systemic fragmentation remain formidable.
The Evolution of the IMD Policy: A Brief Chronology
The "IMD payment exclusion" was codified at the inception of Medicaid to prevent federal funds from being used to support what were then state-run asylums. However, as the opioid epidemic intensified, the rigid nature of this exclusion became a significant barrier to modern addiction medicine.
- 2015: The Centers for Medicare & Medicaid Services (CMS) introduces the first Section 1115 waiver authority for SUD. This signaled a major policy shift, allowing states to receive federal matching funds for short-term stays in IMDs, provided those stays were integrated into a broader, community-based continuum of care.
- 2017: CMS updates the guidance, refining the requirements for states. The new policy emphasized the need for robust care coordination, evidence-based treatment guidelines, and improved access to medications for opioid use disorder (MOUD).
- 2018: The passage of the SUPPORT Act creates a permanent state plan option for limited coverage of IMD services, though few states initially adopted this route compared to the popularity of the 1115 waivers.
- 2024: The Consolidated Appropriations Act makes the SUPPORT Act’s IMD coverage option permanent, further solidifying federal intent to support residential addiction treatment.
- 2026: As of April, 38 states have active SUD IMD waivers, with many now moving into their second five-year cycle of implementation.
Supporting Data: Assessing the Impact of Waivers
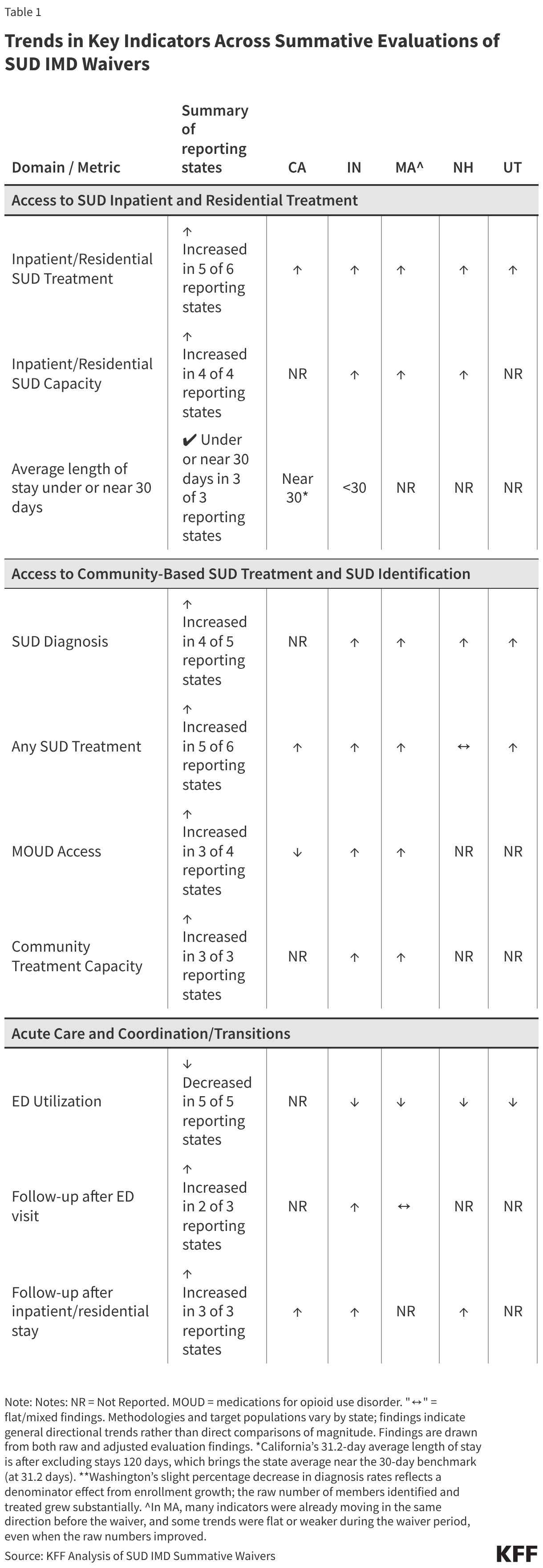
The summative evaluations from six pioneering states—California, Indiana, New Hampshire, Utah, Washington, and Massachusetts—provide the first comprehensive look at how these waivers function in practice. While these findings are considered "directional signals" rather than causal proof due to the concurrent impact of the COVID-19 pandemic and the fentanyl-driven overdose crisis, the data reveals significant trends.
Increased Utilization of Inpatient Care
Evaluations consistently show that states with waivers have successfully increased the volume of residential and inpatient SUD services. By removing the financial barrier to using larger facilities, states were able to expand capacity. In states like California and Indiana, the shift was marked: beds that were previously ineligible for federal reimbursement were suddenly brought under the Medicaid umbrella, allowing for a surge in patient throughput.
Strengthening the Treatment Continuum
The waivers were not intended to favor residential care at the expense of outpatient services. The data indicates that states largely succeeded in this balancing act. In most of the evaluated states, there was a measurable uptick in the number of individuals receiving MOUD and accessing community-based outpatient treatment. The goal of "identifying" SUDs more effectively appears to be working, with more patients entering the system through primary care or emergency department screenings, which are then linked to higher levels of care.
Reducing Acute Care Dependence
One of the primary arguments for the waivers was that better access to residential treatment would reduce the reliance on emergency departments (EDs) for crisis management. The data bears this out: most states reported a decline in SUD-related ED visits. Furthermore, there was a noted, albeit modest, improvement in follow-up care after an acute episode. This suggests that the waivers are helping to bridge the "black hole" of care transitions, where patients often fall through the cracks between the hospital and the recovery center.
Official Perspectives: The Regulatory Landscape
Federal and state officials remain cautiously optimistic but vigilant. The Department of Justice and CMS have both indicated that while residential care is vital, it must never replace the community-based infrastructure that keeps individuals in recovery long-term.
Federal guidance explicitly requires states to demonstrate how their IMD-based care supplements, rather than replaces, community-based options. The recurring concern, as noted by researchers, is that shifting resources toward high-intensity, expensive inpatient care could inadvertently starve community clinics of the funding they need to support long-term recovery.
Moreover, the policy environment is becoming increasingly precarious. The 2025 Reconciliation Law introduced new fiscal restrictions on Medicaid financing, which may challenge the ability of states to maintain the momentum of their mental health and SUD expansions. Policy experts warn that without stable, long-term funding, these "demonstration" programs could become victims of their own success, providing services that the state can no longer afford to sustain once federal waiver authority expires or is tightened.
Implications for the Future of Addiction Medicine
The shift toward covering IMD services has profound implications for how the U.S. addresses addiction, but the evaluations highlight four structural "pain points" that require urgent attention.
1. The Workforce Crisis
Across every evaluated state, the most significant barrier to expansion was not funding, but people. Shortages of licensed clinicians, nurses, and certified addiction counselors mean that even if a facility is authorized to treat more patients, they lack the staff to do so. In rural areas, this is compounded by the lack of local facilities, forcing patients to travel long distances, which inherently weakens the effectiveness of care.
2. Administrative Fragmentation
Stakeholders in states like Utah and California pointed to the "siloed" nature of healthcare financing. When physical health, mental health, and SUD benefits are managed by different entities or under different sets of rules, the result is a fragmented experience for the patient. "Prior authorization" was frequently cited as a major hurdle; even when a state introduces a standardized form, variations in how different managed care plans interpret medical necessity continue to delay care and burden providers with excessive paperwork.
3. The Housing-Treatment Nexus
Perhaps the most sobering finding is the role of housing instability. Clinical teams in multiple states noted that residential treatment is often effective in the short term, but "downward spirals" occur immediately upon discharge if the patient is returned to homelessness. Without adequate transitional housing or recovery residences, the clinical gains made in an IMD are often lost within weeks.
4. Defining "Success" in an Era of Fentanyl
Finally, the impact on overdose deaths remains the most elusive metric. The evaluation reports found that despite expanded access to treatment, overdose death rates often remained stagnant or continued to rise during the study period. This is largely attributed to the lethality of the illicit fentanyl supply, which has outpaced the gains made in treatment access. This suggests that while Medicaid waivers are a necessary component of the solution, they are not a silver bullet against a rapidly evolving toxic drug supply.
Conclusion
The transition toward allowing Medicaid to pay for inpatient and residential SUD treatment is a landmark development in American social policy. It acknowledges that for many, recovery begins in a facility, not on the street. However, the first wave of summative evaluations proves that the "waiver" is only the beginning.
To turn these policies into long-term public health success, states must move beyond merely filling beds. They must focus on the "post-discharge" ecosystem, streamlining administrative hurdles for providers, and investing in the workforce necessary to deliver care. As the U.S. continues to navigate the complexities of the addiction crisis, these Section 1115 waivers serve as a vital, if imperfect, laboratory for building a more responsive, integrated, and effective system of behavioral healthcare.