In the intricate landscape of the United States healthcare system, a distinct group of 12 million Americans exists at the intersection of two massive federal and state programs: Medicare and Medicaid. Known as "dual-eligible individuals," these beneficiaries occupy a unique, often precarious position. Because they navigate two separate bureaucracies to manage their health, they are frequently subject to fragmented care, administrative hurdles, and significantly higher health risks compared to those who rely on only one program.
A new, comprehensive analysis of 2022 and 2023 administrative claims data sheds light on this population, revealing that their health outcomes and the associated fiscal impact on the U.S. economy are far more profound than previously understood. By analyzing the interplay between chronic disease prevalence and government spending, this report highlights the urgent need for structural reform in how we coordinate care for the nation’s most vulnerable patients.
Main Facts: Who are the Dual-Eligible?
The dual-eligible population is not monolithic; it is divided into two primary categories based on the level of assistance they receive.
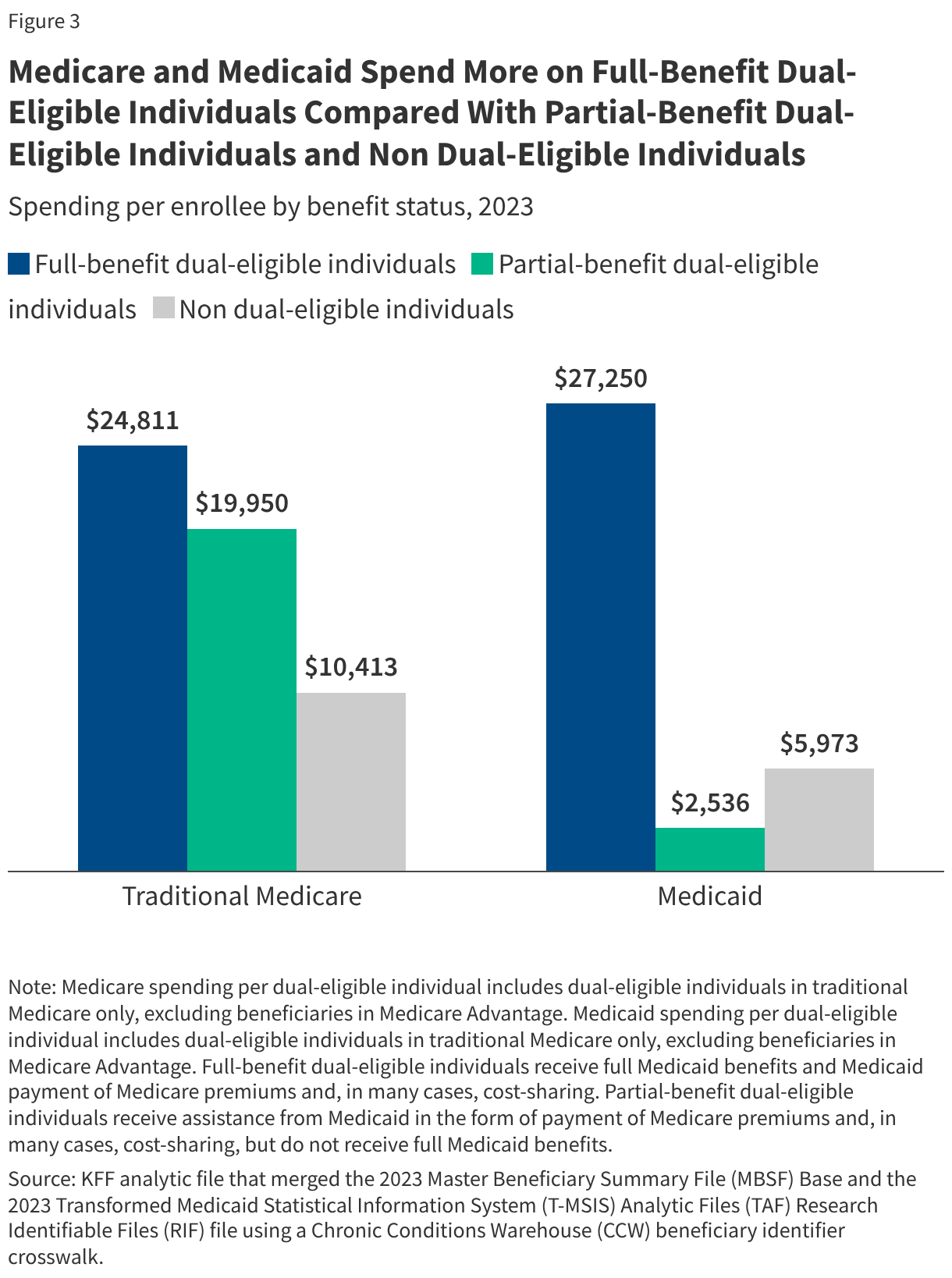
Of the 12 million dual-eligibles, approximately 8.6 million are classified as "full-benefit" individuals. These are individuals who qualify for Medicaid benefits beyond the basic Medicare coverage—including essential services like long-term care, dental, vision, and hearing aids. The remaining 3.5 million are "partial-benefit" enrollees. These individuals primarily receive help with Medicare premiums and cost-sharing through the Medicare Savings Programs (MSPs).
For this group, the division of labor is clear yet often disjointed: Medicare serves as the primary payer for medical and post-acute care, while Medicaid functions as a "wraparound" insurer, covering the out-of-pocket costs that would otherwise be prohibitive. However, the administrative burden of managing two distinct insurance cards often leads to disjointed care, where communication between providers, pharmacies, and specialists fails to bridge the gap between the two systems.
Chronology of Systemic Fragmentation
The dual-eligible challenge is not new, but it has intensified over the last two decades as the U.S. population ages and the cost of chronic disease management skyrockets.
- Early 2000s: The implementation of Medicare Part D brought prescription drug coverage to the dual-eligible population, but the transition from state-based pharmacy programs to federal coverage highlighted the difficulties of integrating disparate insurance systems.
- 2010s: The Affordable Care Act and the subsequent creation of the Medicare-Medicaid Coordination Office (MMCO) signaled a shift toward "integrated care models," attempting to combine Medicare and Medicaid benefits into a single managed care plan.
- 2020-2022: The COVID-19 pandemic exacerbated the vulnerabilities of the dual-eligible population. With higher rates of underlying chronic conditions, this group faced higher hospitalization and mortality rates, leading to a surge in utilization of both long-term services and acute hospital care.
- 2023-Present: The latest administrative data indicates that despite policy efforts to integrate care, the fiscal and clinical burden remains disproportionately high, with chronic disease management serving as the primary driver of rising costs.
Supporting Data: The Fiscal and Clinical Weight
The data reveals a stark reality: dual-eligible individuals represent a small slice of the overall population but account for an outsized portion of total healthcare spending.
1. Disproportionate Spending Shares
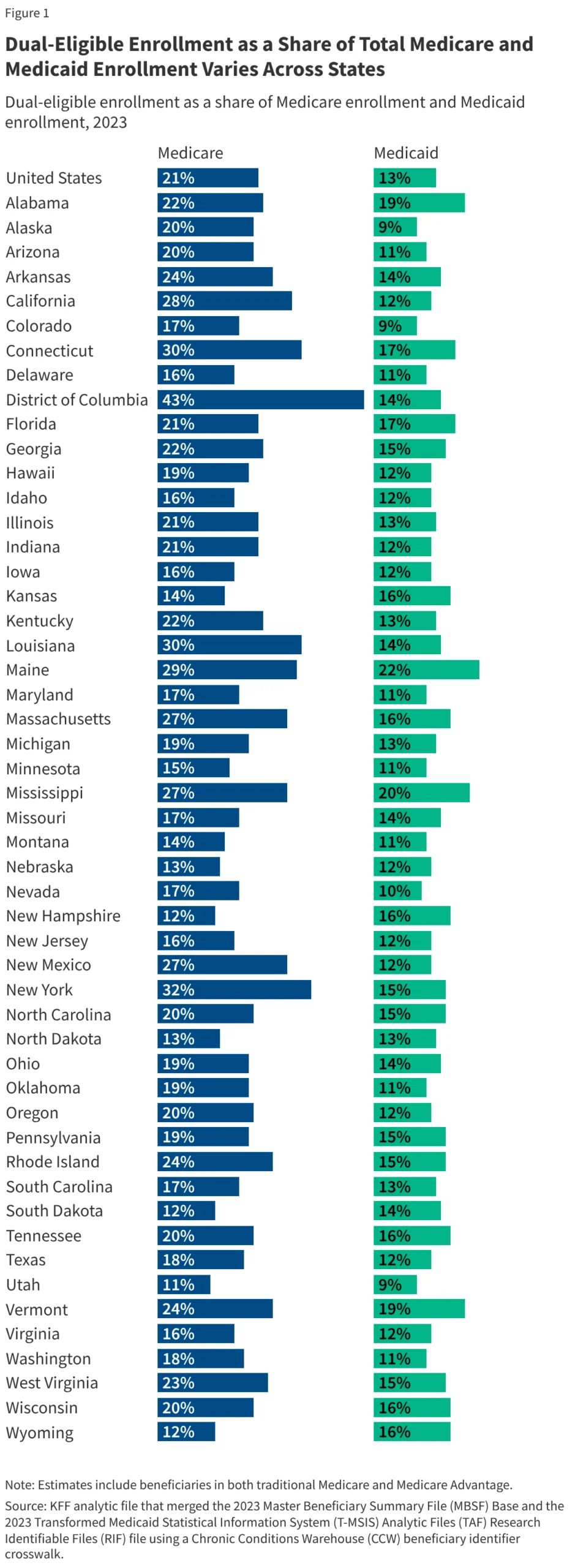
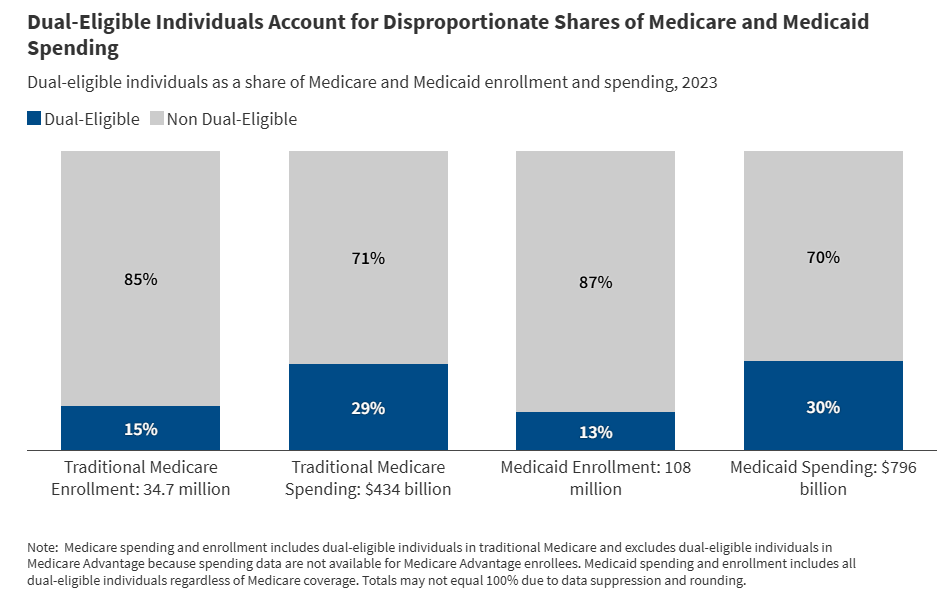
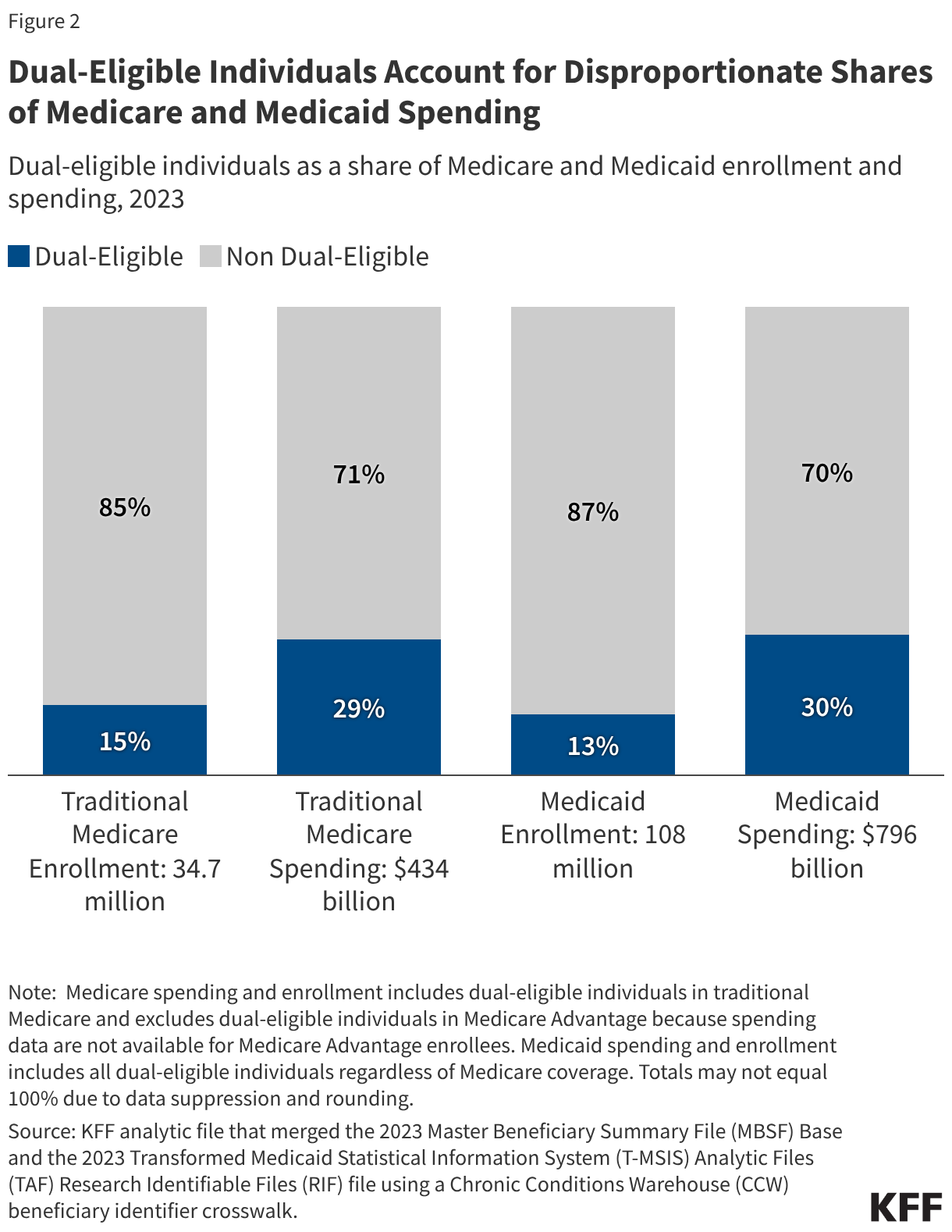
Nationally, dual-eligible individuals make up 21% of the Medicare population and 13% of Medicaid enrollees. Despite these relatively modest figures, they account for 29% of traditional Medicare spending—amounting to roughly $127 billion—and a staggering 30% of total Medicaid spending ($241 billion). This "spend-to-enrollment" gap is fueled by the higher per-person intensity of care required for this demographic.
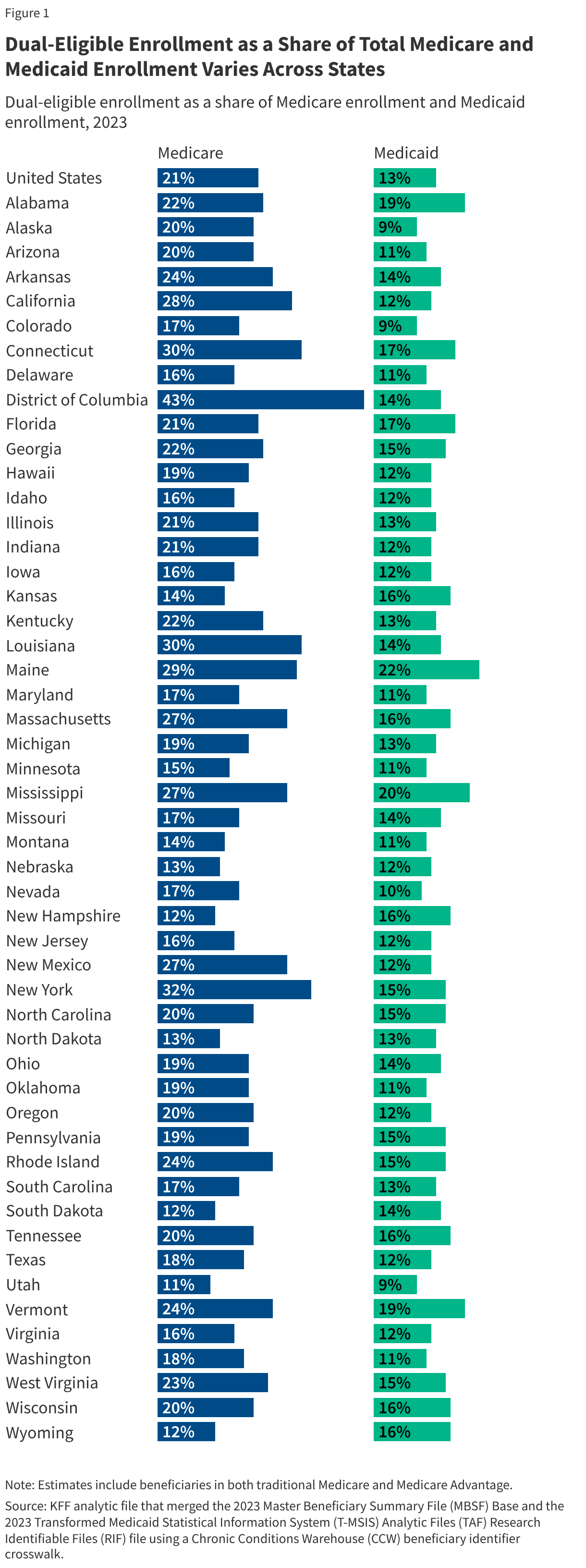
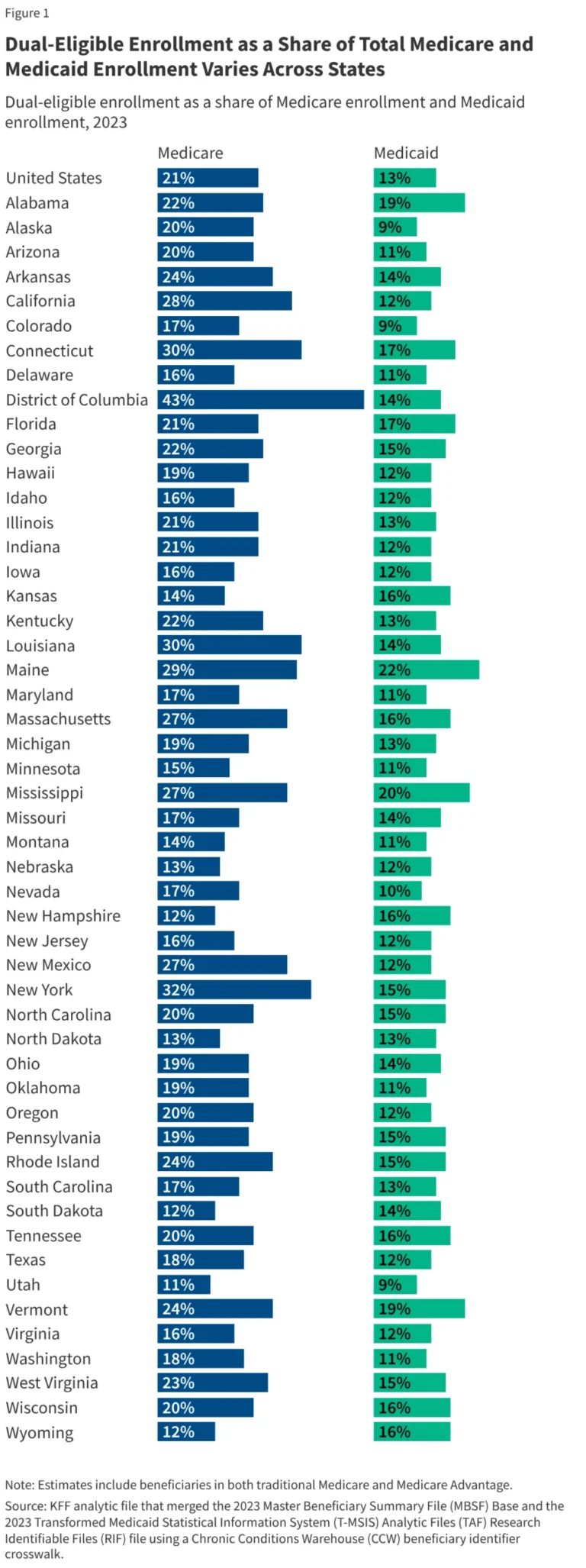
2. State-Level Variability
The concentration of dual-eligibles varies significantly by geography, driven by state-specific Medicaid eligibility policies and demographic factors. In the District of Columbia, New York, Connecticut, and Louisiana, dual-eligibles account for 30% or more of the Medicare population. Conversely, in states like Utah, the share is as low as 11%. This variation underscores how state policy, rather than just clinical need, dictates access to the wraparound support services that can improve long-term outcomes.
3. The Chronic Condition Multiplier
Perhaps the most telling data point is the prevalence of chronic disease. Fifty-seven percent of full-benefit dual-eligibles suffer from five or more chronic conditions. In stark contrast, only 2% of "Medicaid-only" enrollees (who are typically younger) manage five or more chronic conditions.
The financial impact of these conditions is linear and severe: a dual-eligible individual with no chronic conditions incurs roughly $3,955 in traditional Medicare costs. For an individual with five or more chronic conditions, that number balloons to $40,341. When Medicaid spending for long-term care is added to this equation, the fiscal burden for the most complex patients reaches astronomical levels.
Official Responses and Policy Perspectives
Healthcare policymakers and advocates remain divided on the best path forward. Some argue that moving all dual-eligibles into fully integrated managed care plans is the solution, as it would theoretically provide a single point of accountability for a patient’s medical, behavioral, and long-term care needs.
"The current system forces patients to act as their own case managers," notes a senior policy analyst at the Kaiser Family Foundation. "When you have one insurance provider for your doctor visits and another for your long-term nursing care, the patient falls into the gap. We are paying a premium for a system that is inherently inefficient."
Conversely, some patient advocacy groups express concern that aggressive integration could limit the choice of providers or restrict access to specialized services if the managed care entities are incentivized to cut costs. The federal government, through the MMCO, continues to incentivize states to test "demonstration projects," yet large-scale adoption of unified, integrated care remains inconsistent across the U.S.
Implications: The Path Toward Reform
The data presented in the 2022-2023 analysis serves as a wake-up call for federal and state health officials. The implications of these findings are threefold:
1. The Need for Proactive Care Management:
Because spending increases exponentially with the number of chronic conditions, early intervention is the only viable path to cost containment. Moving away from a reactive "fee-for-service" model toward a proactive, multidisciplinary care model—where primary care physicians, social workers, and geriatric specialists communicate in real-time—is essential.
2. Addressing the Long-Term Care Gap:
Medicare’s historical refusal to cover long-term, custodial care is the single biggest driver of the "split-coverage" problem. As long as Medicare focuses on acute medical events and Medicaid covers the chronic, daily living support, the two systems will remain in a tug-of-war. Policy proposals to integrate long-term services and supports (LTSS) into a more comprehensive Medicare benefit package could alleviate the financial pressure currently placed on state Medicaid budgets.
3. Data-Driven Resource Allocation:
The wide variation in enrollment and spending across states suggests that some states have developed more efficient systems for identifying and supporting their dual-eligible populations. Federal regulators must look at the best practices in states with higher integration rates and provide the funding mechanisms necessary to replicate these models in states where the dual-eligible population remains underserved.
Conclusion
The 12 million dual-eligible Americans represent the most complex, cost-intensive, and vulnerable demographic in the U.S. healthcare system. They are the individuals for whom the promise of the social safety net is tested most severely. As the population continues to age, the incidence of multiple chronic conditions will only rise, putting further strain on an already fragmented system.
Reform cannot wait. By recognizing the direct link between chronic disease, the need for long-term support, and the administrative failure of disjointed insurance, policymakers have the opportunity to transition from a system of overlapping bureaucracy to one of integrated, patient-centered care. The fiscal health of the Medicare and Medicaid programs depends on it, but more importantly, the dignity and quality of life of millions of Americans depend on the system finally working for them, rather than against them.