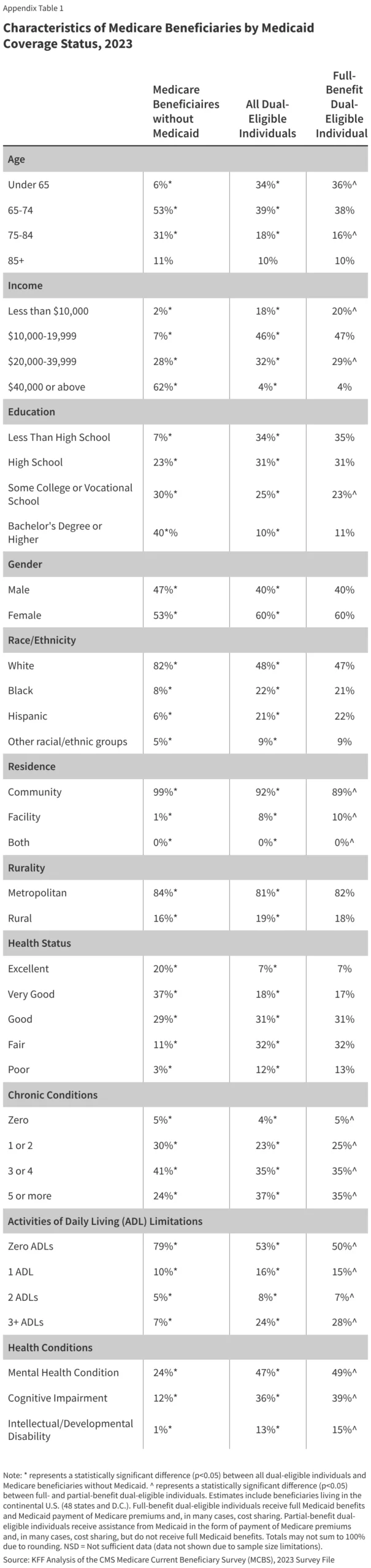
For the 1.2 million older adults and younger individuals with disabilities residing in America’s 14,700 nursing homes, the quality of daily care is not merely a policy metric—it is a matter of life and death. Recent data from the Department of Health and Human Services (HHS) underscores the magnitude of this reality: more than one-third of all adults will utilize some form of nursing home care after reaching the age of 65. Yet, as the nation navigates a shifting landscape of federal oversight, questions regarding the safety, clinical standards, and accountability of these facilities have reached a critical inflection point.
The Foundation of Oversight: A Federal-State Partnership
To ensure that vulnerable populations receive adequate care, the U.S. healthcare system relies on a complex, federal-state partnership. Nursing homes seeking federal funding through Medicare or Medicaid must adhere to stringent "conditions of participation." These standards mandate that facilities provide not only basic shelter but clinical care, medical treatment, and a safe environment for daily living.
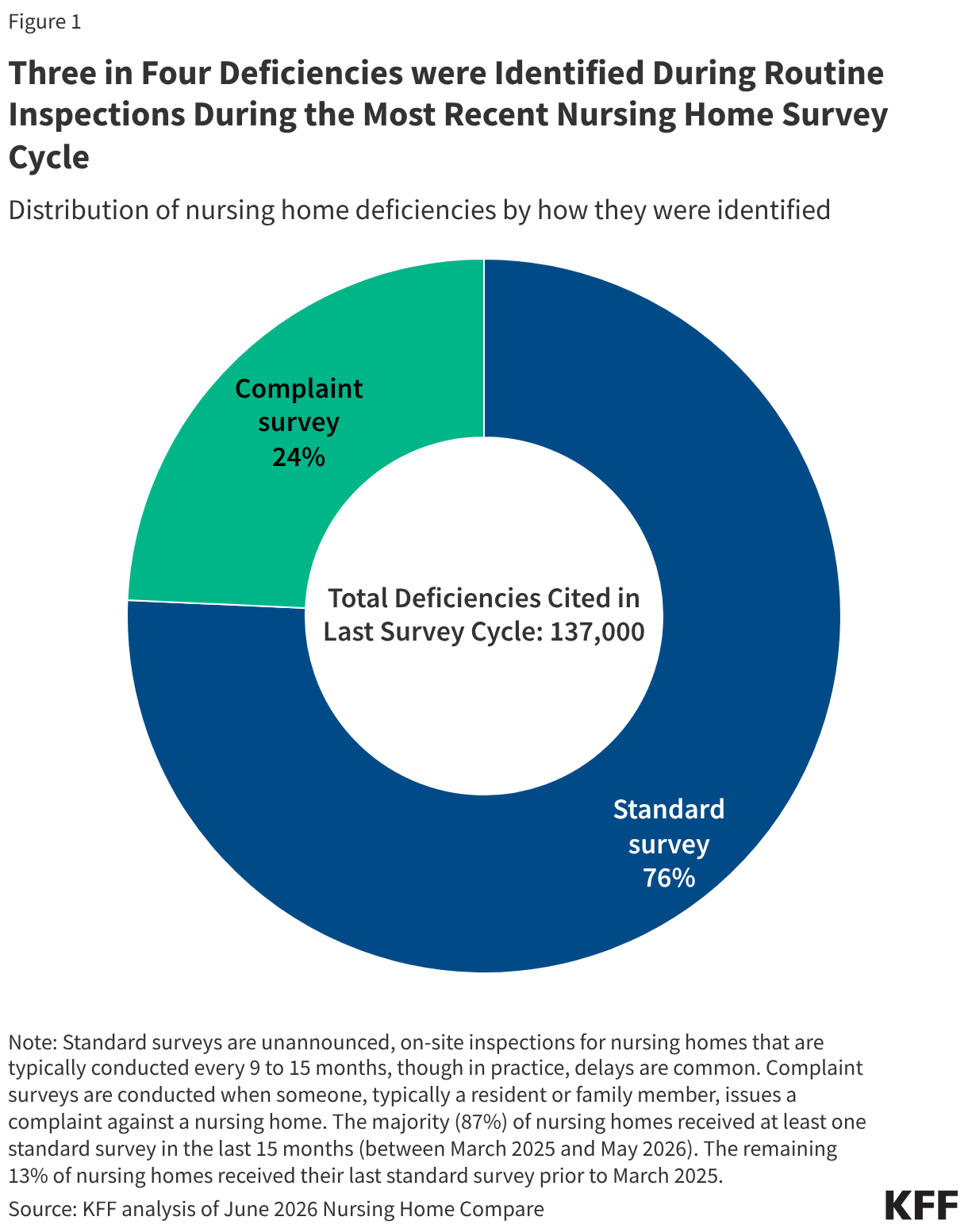
The mechanism for enforcing these standards is the unannounced, on-site inspection—or "standard survey." Administered by state agencies in coordination with the Centers for Medicare & Medicaid Services (CMS), these surveys are the primary filter for catching systemic failures. When a facility fails to meet a federal requirement, inspectors issue a "deficiency." While these surveys are intended to be routine, they are frequently supplemented by "complaint surveys," which are triggered when residents, family members, or staff report specific instances of neglect or abuse.
A Shifting Regulatory Landscape
The integrity of the nursing home inspection process has been subject to intense debate, particularly following shifts in federal policy during the Trump administration. These changes included the rescission of the Biden-era nursing home staffing rule, a pivot toward prioritizing complaint-based inspections over routine surveillance, and the suspension of deadlines for reporting detailed ownership information.
Furthermore, administrative challenges have compounded the difficulty of oversight. In May 2026, CMS issued guidance to state directors noting a reduction in federal "validation inspections"—on-site monitoring meant to ensure state agencies are accurately reporting facility conditions. This reduction was attributed to the 2025 federal government shutdown, which created a backlog of work and limited the capacity for federal oversight.
Chronology of Inspection Compliance
Federal law mandates that every nursing home undergo a standard survey at least once every nine to fifteen months. However, the reality of execution often falls short of the ideal.
- Current Status: As of mid-2026, roughly 87% of nursing homes have successfully received a standard survey within the last 15 months.
- The Lag: Approximately 10% of facilities were surveyed between January 2024 and February 2025, leaving a concerning 3% of facilities that have not undergone a standard survey since prior to 2024.
This variability in inspection frequency often correlates with staffing shortages and the discretionary flexibility granted to states, which allows them to focus resources on facilities with historical quality issues while potentially neglecting others.
Data-Driven Insights: Quantifying the Failures
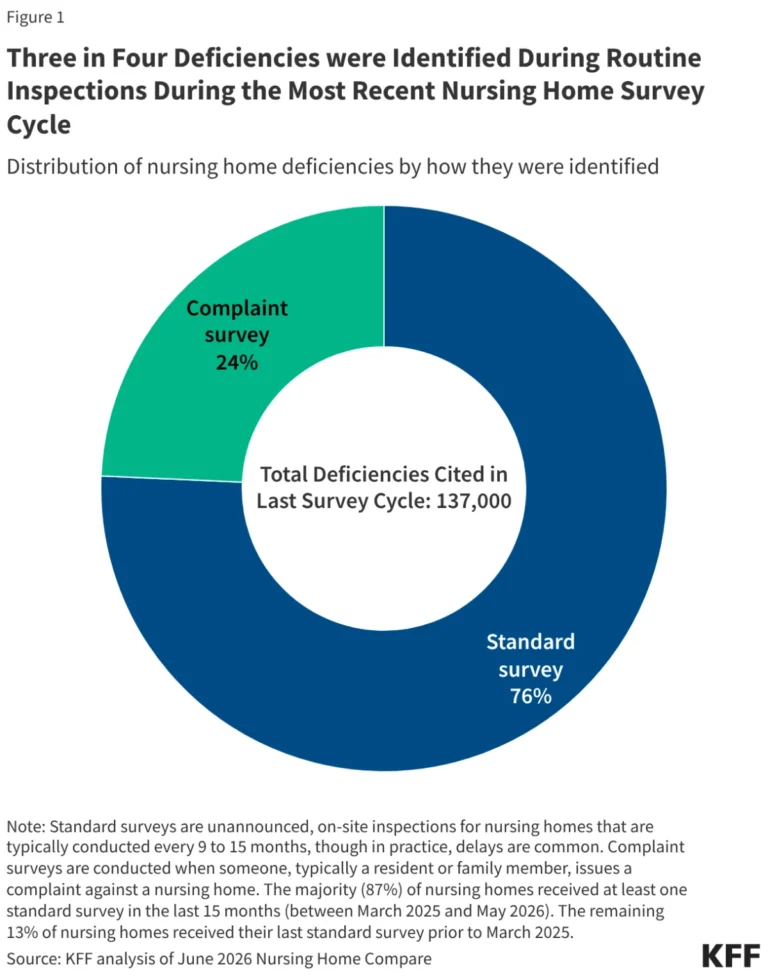
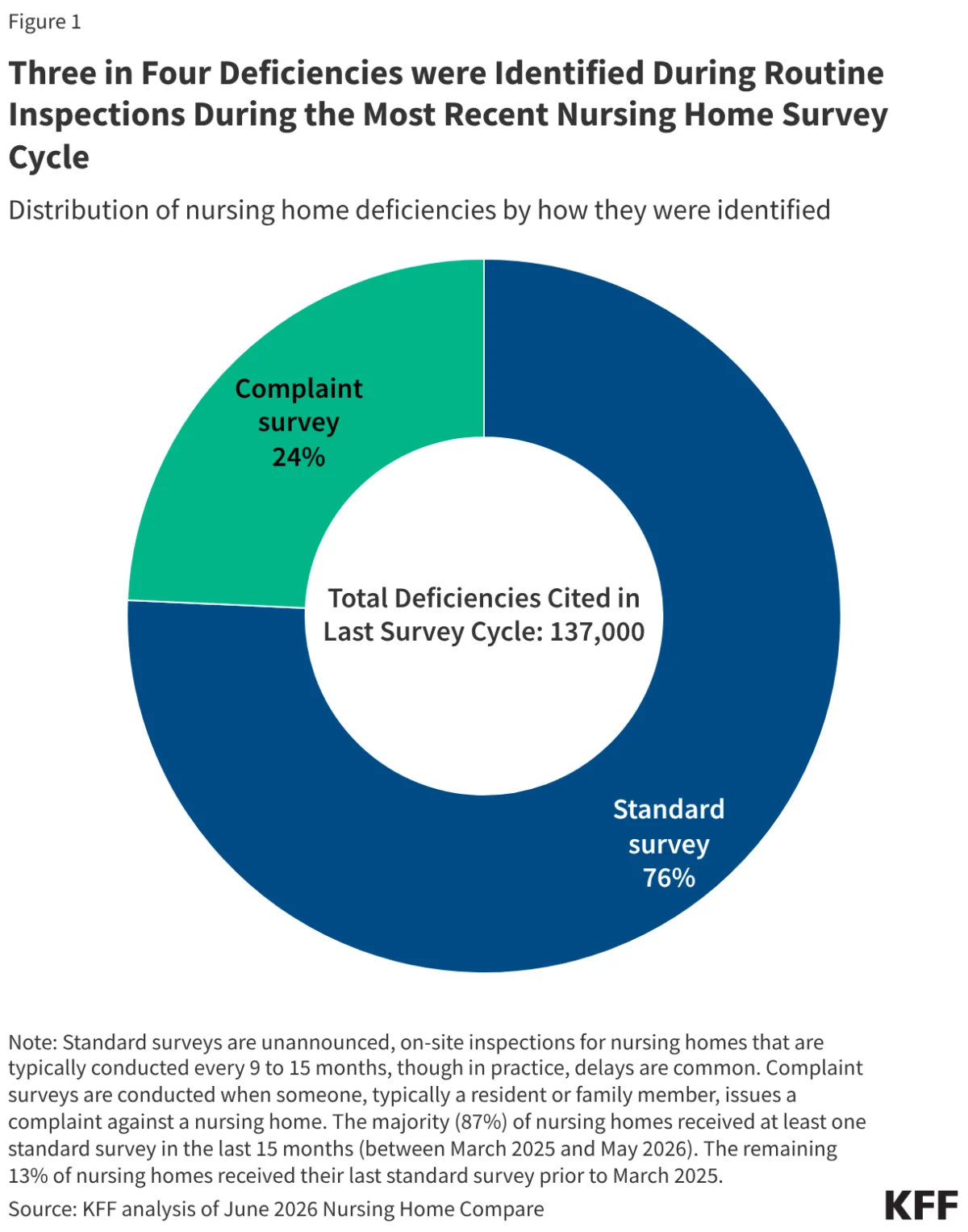
An analysis of data from Nursing Home Compare reveals that roughly one in four nursing home deficiencies are identified through complaint-based surveys, while the remaining three-quarters are identified during routine standard surveys.
Understanding Scope and Severity
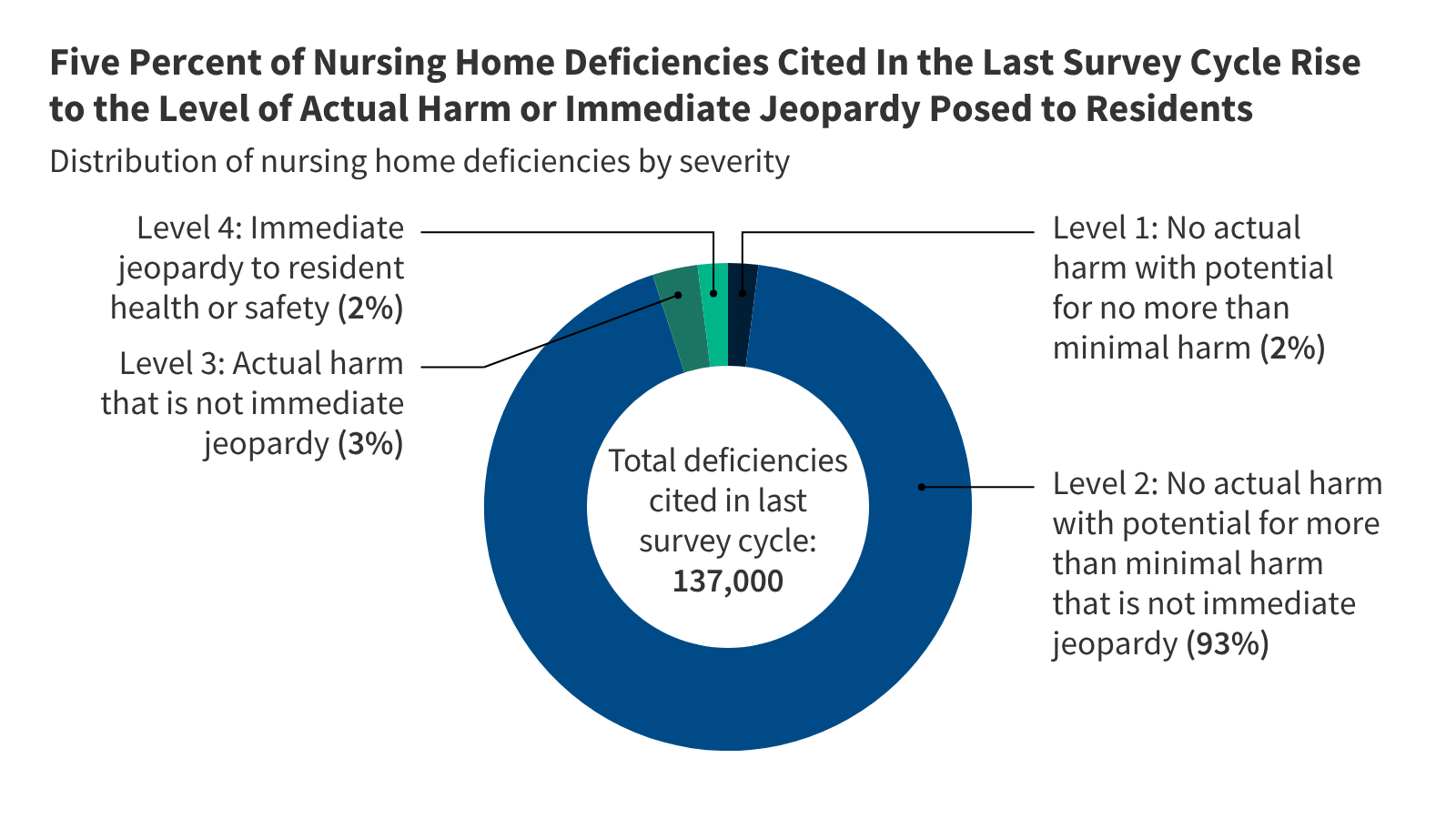
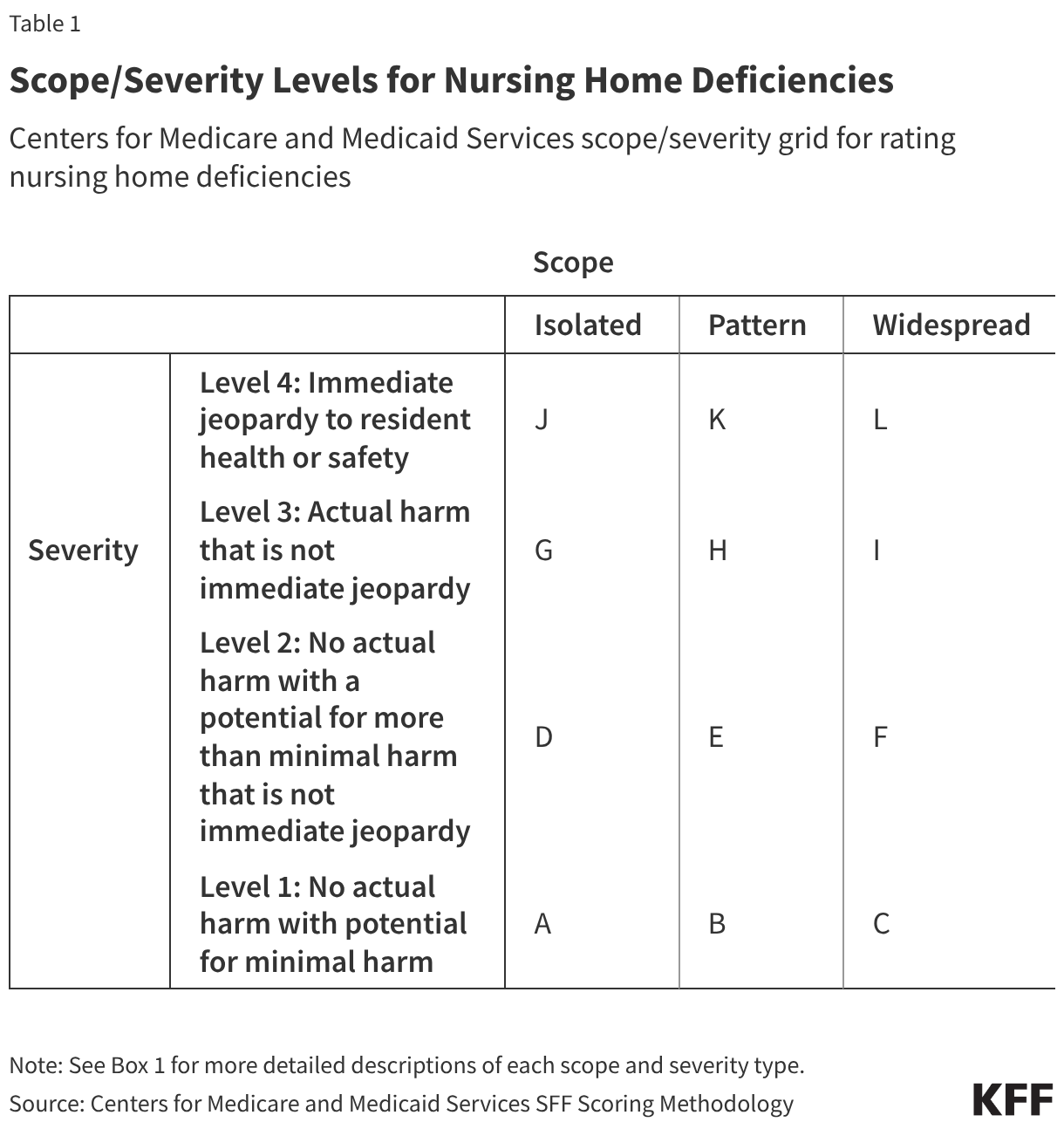
CMS categorizes these failures using a "Scope and Severity" matrix (A through L).
- Scope refers to how widespread the issue is, ranging from "Isolated" (one resident) to "Widespread" (systemic failure).
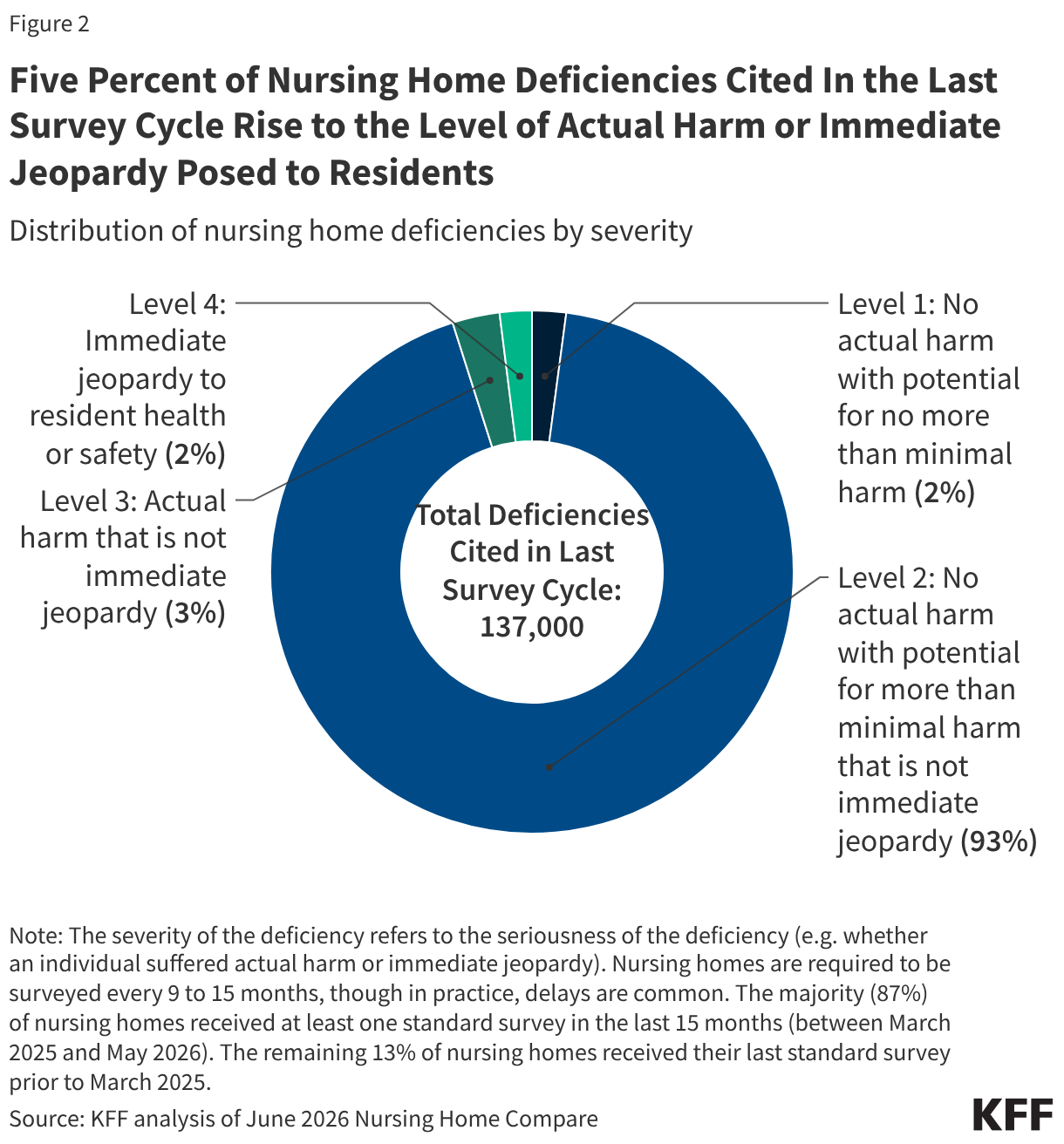
- Severity ranges from Level 1 (minimal harm) to Level 4 (Immediate Jeopardy).
"Immediate Jeopardy" (Level 4) is the most critical classification, reserved for situations where a facility’s noncompliance has caused, or is likely to cause, serious injury, harm, or death. While only about 5% of all cited deficiencies rise to Level 3 or 4, these categories represent the most egregious failures in clinical duty.
The Human Cost: Examples from the Field
The consequences of these deficiencies are tangible. Reports from the most recent survey cycle include harrowing instances of systemic neglect:
- Failure of Safety Protocols: One facility failed to secure a bedside rail, resulting in a resident falling and suffering a fractured femur.
- Clinical Neglect: Another facility failed to provide necessary respiratory care for a resident, leading to a prolonged, agonizing delay in treatment that resulted in a pneumonia and influenza diagnosis.
- Nutritional and Dietary Failures: Reports cite facilities failing to provide nectar-thick liquids to residents with swallowing difficulties, directly risking aspiration, as well as failures to track basic nutritional status or weight, leading to unmonitored health decline.
The Staffing Correlation
Perhaps the most significant finding in the latest analysis is the direct link between staffing levels and facility quality. The data is stark: nursing homes with low staffing levels are significantly more likely to report severe (Level 3 or 4) deficiencies than their well-staffed counterparts.
Specifically, 32% of low-staffing facilities reported Level 3 deficiencies, compared to only 18% in high-staffing homes. The disparity is even more pronounced at Level 4, where low-staffing facilities were nearly three times more likely to be cited for immediate threats to life and safety (27% vs. 10%). Furthermore, low-staffing facilities are disproportionately prone to systemic, widespread failures, suggesting that understaffing is not merely a matter of convenience, but a fundamental driver of poor clinical outcomes.
Official Responses and Policy Implications
The current oversight model faces a dual challenge: the necessity of enforcing federal standards and the logistical reality of state-level implementation. Proponents of stronger regulation argue that the reliance on "complaint-driven" inspections is inherently reactive, effectively waiting for harm to occur before taking action.
Conversely, some industry stakeholders suggest that the administrative burden of frequent inspections can strain resources in rural and underfunded facilities. However, the data strongly suggests that the absence of regular, rigorous oversight allows low-staffing patterns to go unchecked, creating a feedback loop of declining quality.
Addressing the Future
The implications for policymakers are clear:
- Staffing Mandates: The data provides a strong empirical basis for reinstating and enforcing robust minimum staffing standards, as these are the single most effective buffer against severe quality deficiencies.
- Increased Validation: CMS must prioritize the restoration of Federal Monitoring Surveys to ensure that state agencies are maintaining consistency and accuracy in their reporting.
- Transparency: As ownership structures in nursing homes become increasingly complex—often involving private equity and real estate investment trusts—the suspension of reporting deadlines must be reversed to allow for full public and regulatory visibility.
Conclusion
The nursing home industry stands at a crossroads. While the vast majority of deficiencies fall into the "potential for harm" category rather than "actual harm," the existence of systemic, widespread failures in understaffed facilities cannot be ignored. As the aging population grows, the demand for high-quality, safe, and accountable nursing care will only intensify. Ensuring that the "survey and certification" process is not just a bureaucratic checkbox, but a robust safeguard for the most vulnerable, must remain a top priority for federal and state health departments.
For the families of the 1.2 million residents currently in care, the promise of quality is not a luxury; it is the fundamental expectation of a society that values the dignity and safety of its elderly and disabled citizens. The data is clear—now, the policy response must match the urgency of the crisis.