In the complex landscape of American healthcare, the programs of Medicare and Medicaid serve as the primary lifelines for tens of millions. While Medicare provides the bedrock of coverage for seniors and those with disabilities, and Medicaid serves as the nation’s largest public health insurance safety net for low-income populations, there exists a critical group that relies on both. These individuals, known as "dual-eligible" beneficiaries, sit at the intersection of two massive federal systems. With the 2025 budget reconciliation law now introducing significant fiscal shifts, the stability and health outcomes of these 12 million Americans are facing a period of profound uncertainty.
Main Facts: Who Are the Dual-Eligible?
Dual-eligible individuals are beneficiaries who receive primary health insurance through Medicare while simultaneously receiving additional financial and service-based assistance from their state Medicaid programs. This population is generally categorized into two distinct groups based on their level of coverage:
- Full-Benefit Dual-Eligibles (Approx. 9 million): These individuals qualify for Medicaid benefits that Medicare does not cover, such as long-term care, dental, vision, and hearing services. They are often the most economically and medically vulnerable.
- Partial-Benefit Dual-Eligibles (Approx. 3 million): These individuals receive assistance primarily through the Medicare Savings Programs, which help cover Medicare premiums and, in many cases, cost-sharing requirements.
These individuals are not a monolithic group. They represent the most medically complex and economically disadvantaged segment of the Medicare population, often requiring a sophisticated coordination of care that the current, fragmented federal-state system struggles to provide.
Chronology of a Shifting Landscape
The policy environment for these beneficiaries has shifted dramatically in recent years, culminating in the 2025 budget reconciliation law. To understand the current climate, one must look at the progression of these programs:
- Pre-2023: The dual-eligible population remained a focus of legislative efforts to "integrate" care, aimed at reducing the administrative friction between Medicare’s federal oversight and Medicaid’s state-based management.
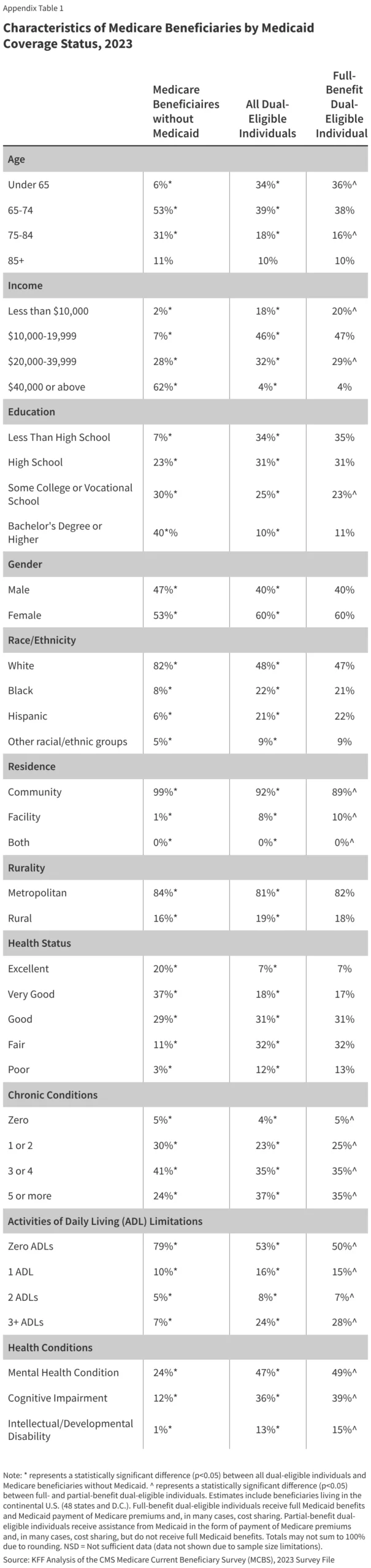
- 2023: The Medicare Current Beneficiary Survey (MCBS) captured a detailed snapshot of this population, highlighting deep disparities in health status and socioeconomic standing compared to those on Medicare alone.
- 2025: The enactment of the federal budget reconciliation law marked a turning point. The law introduced significant reductions in future federal Medicaid spending.
- Post-2025 Outlook: Analysts anticipate that these spending reductions will lead to a decrease in the total number of low-income beneficiaries eligible for the dual-enrollment program. Furthermore, as states face the fiscal pressure of federal budget tightening, many are expected to trim "optional" Medicaid benefits—the very services (like dental and long-term care) that many full-benefit dual-eligibles rely on to survive.
Supporting Data: A Demographic and Health Profile
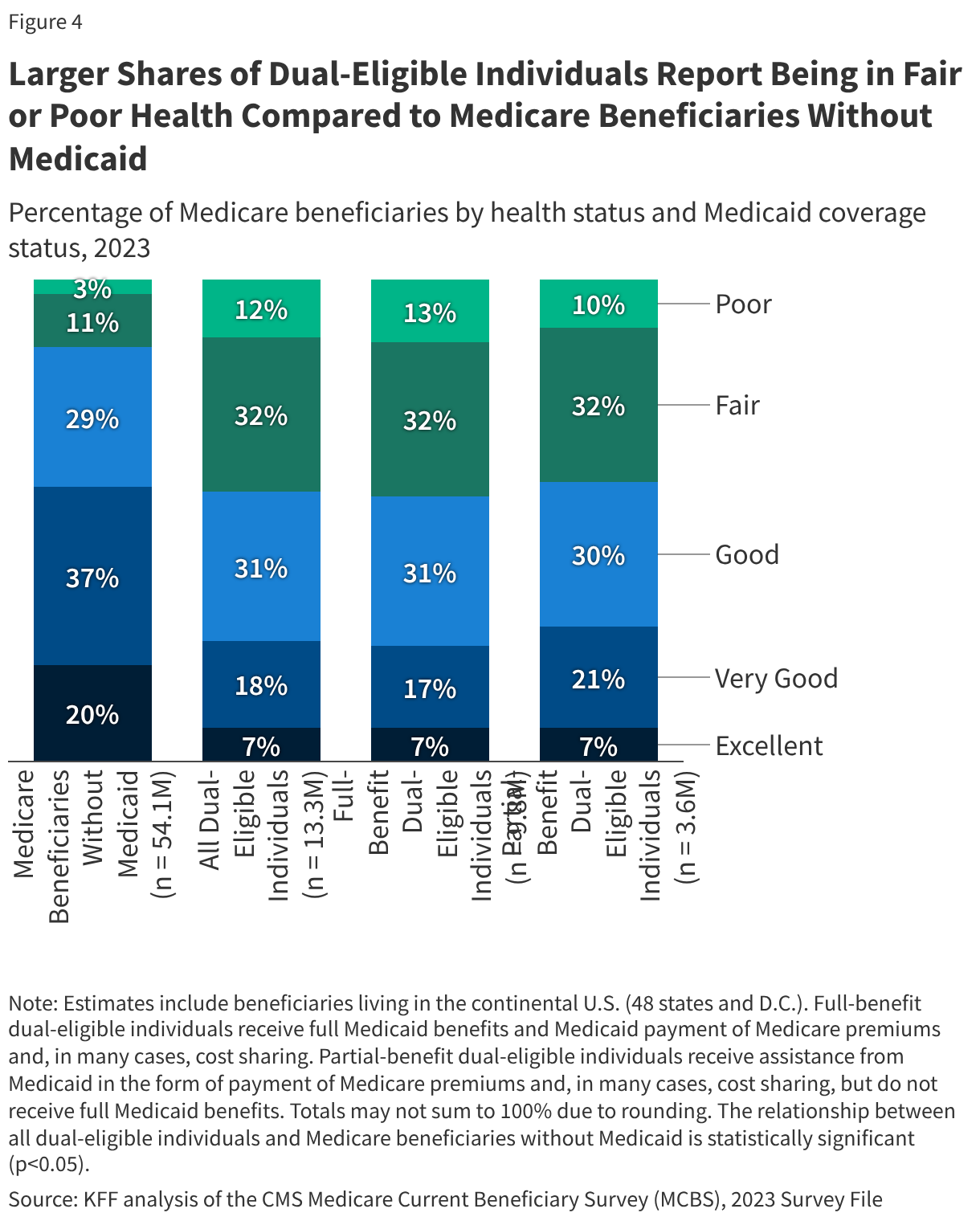
Data from the 2023 MCBS reveals a stark contrast between dual-eligible individuals and those enrolled in Medicare alone. The disparities are not merely financial; they are deeply ingrained in the physical and mental health realities of the population.
Socioeconomic Barriers
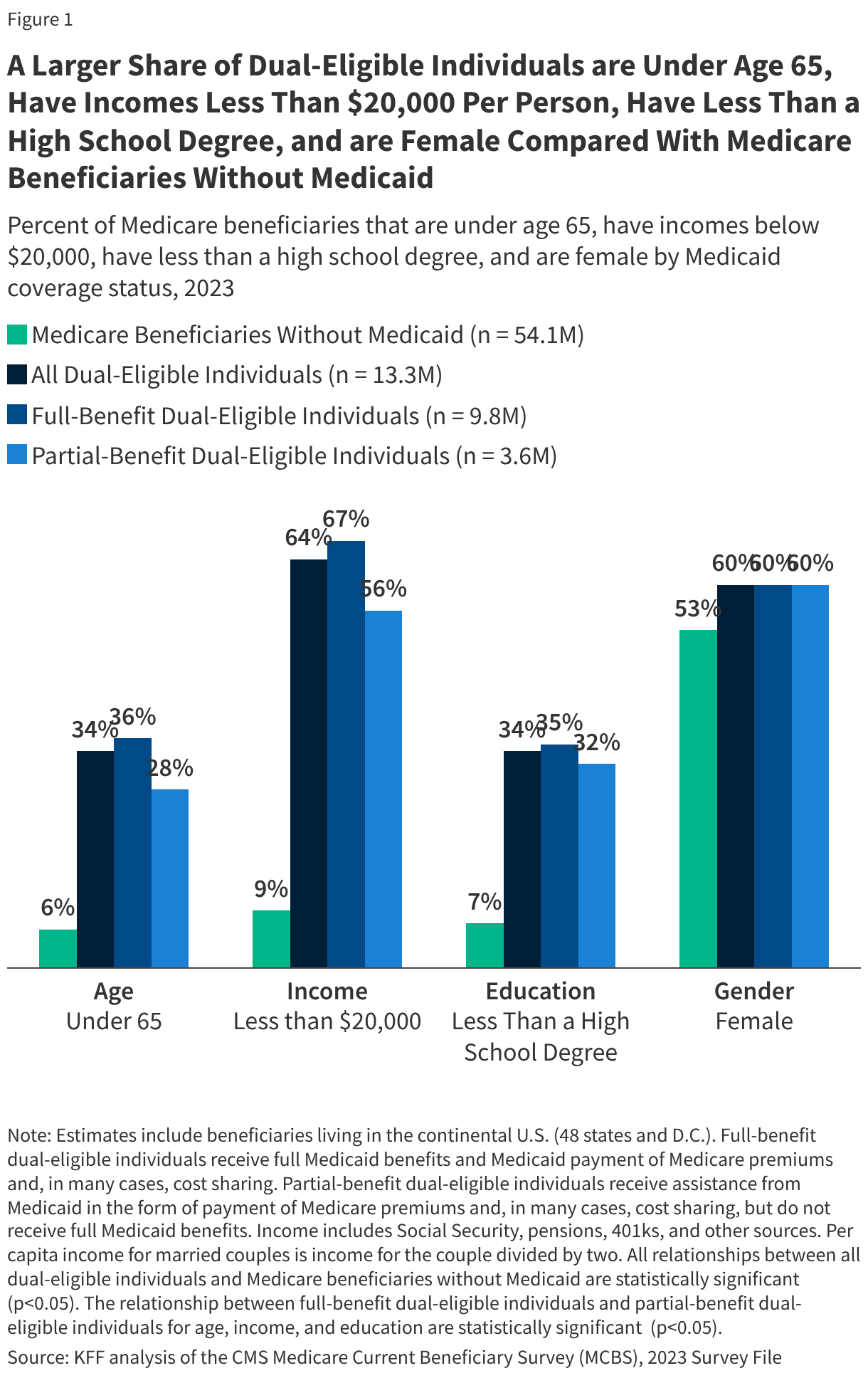
The financial divide is cavernous. Nearly two-thirds (64%) of dual-eligible individuals live on an annual income of less than $20,000. In contrast, only 9% of Medicare beneficiaries without Medicaid fall into this income bracket. Education levels further illustrate this gap, with over one-third (34%) of dual-eligibles lacking a high school diploma, compared to just 7% of their non-Medicaid counterparts.
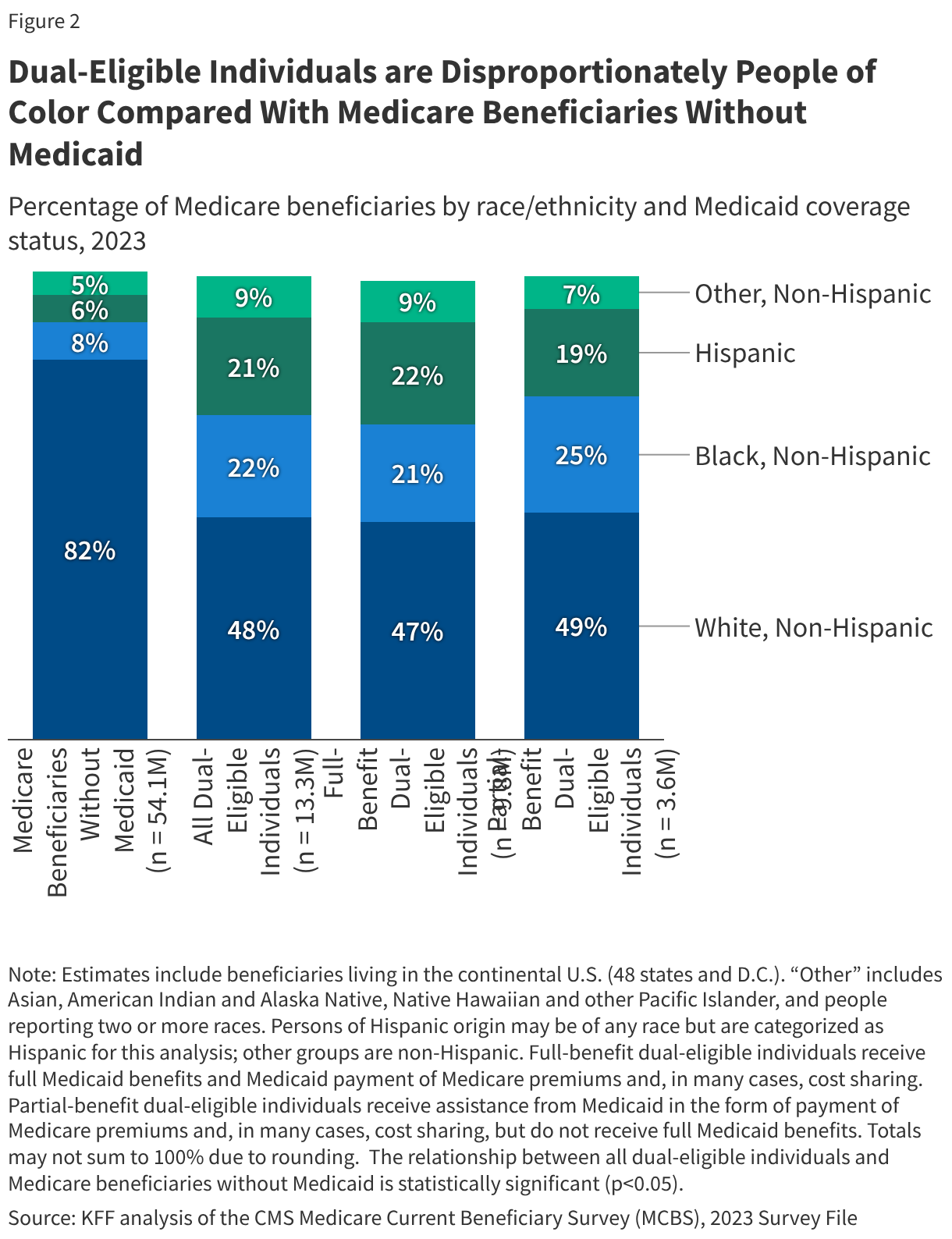
Demographic Disproportionality
The dual-eligible population is significantly more diverse than the broader Medicare population. They are disproportionately people of color: 22% identify as Black and 21% as Hispanic, compared to 8% and 6%, respectively, among those without Medicaid. Additionally, 34% of dual-eligibles are under the age of 65, qualifying for Medicare due to long-term disabilities, whereas only 6% of the non-Medicaid Medicare population falls into this younger category.
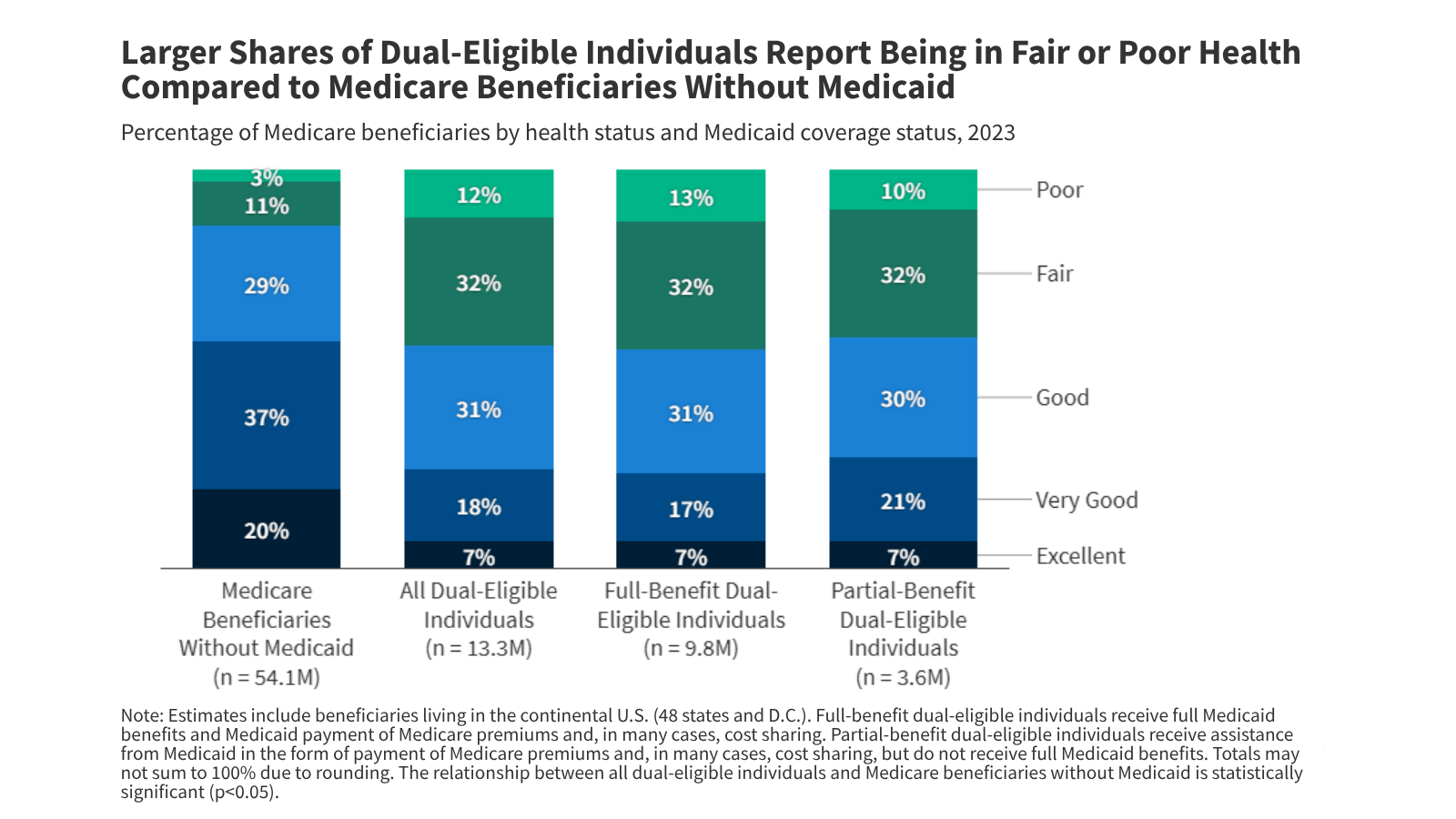
Health and Institutionalization
The health status of this group is markedly worse. While 57% of Medicare-only beneficiaries report being in "very good" or "excellent" health, only 25% of dual-eligibles say the same.
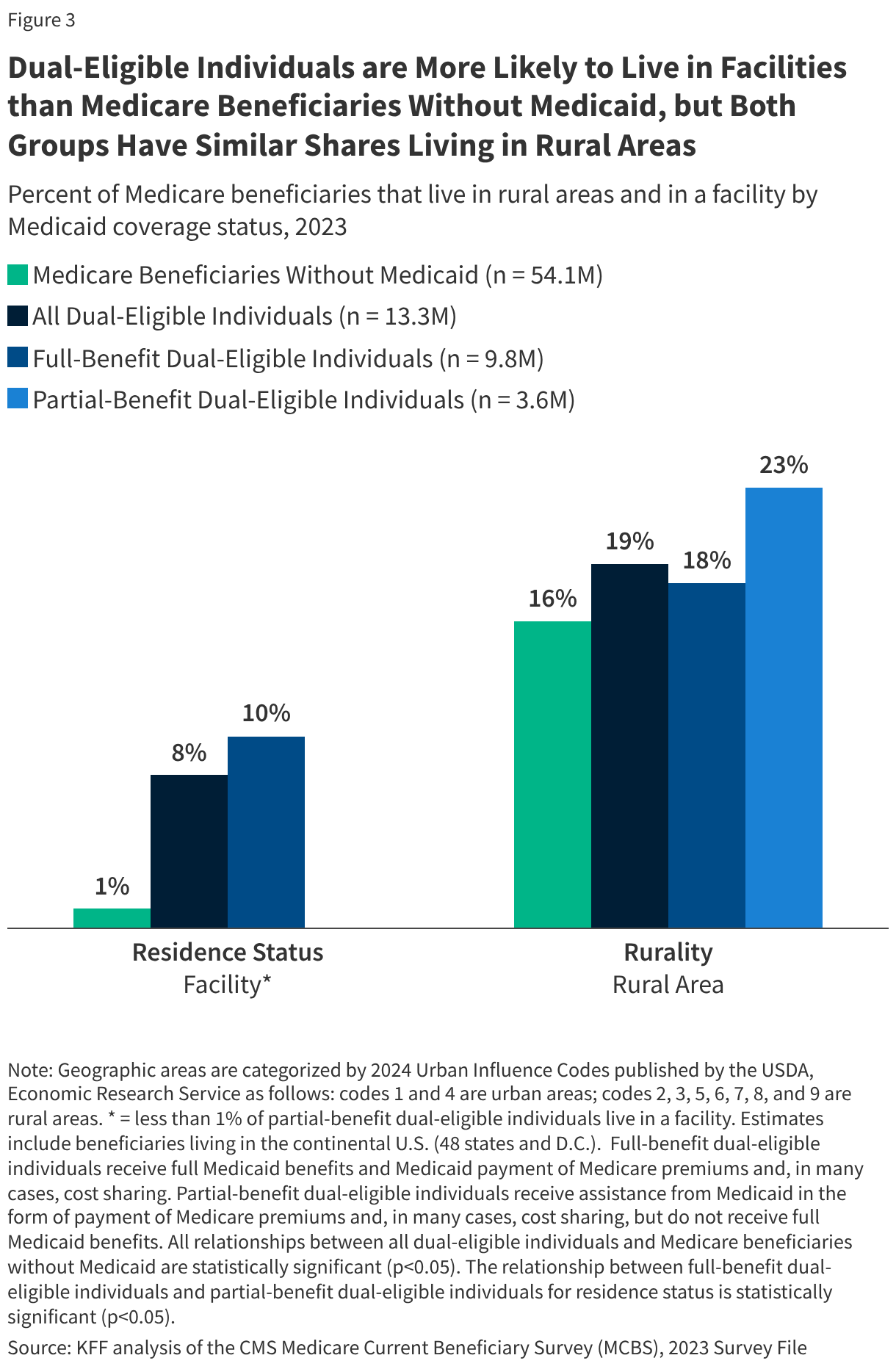
Perhaps most striking is the reliance on institutional care. Approximately 10% of full-benefit dual-eligible individuals live in nursing homes or similar facilities. With the average cost of a private room in a nursing facility exceeding $116,800 in 2023, Medicaid has become the nation’s primary payer for long-term care. Without this coverage, the financial barrier to basic survival for these individuals would be insurmountable.
Mental and Cognitive Hurdles
The burden of disease is also significantly higher among this group:
- Mental Health: 47% of dual-eligibles report a mental health condition (such as depression), compared to 24% of Medicare-only beneficiaries.
- Cognitive Impairment: 36% of dual-eligibles face challenges with concentration, memory, or decision-making, compared to 12% of others.
- Developmental Disabilities: 13% of dual-eligibles report intellectual or developmental disabilities, compared to just 1% of the non-Medicaid Medicare population.
Official Responses and Policy Perspectives
Advocates for the elderly and disabled have expressed significant alarm regarding the 2025 budget law. Policy analysts at organizations like KFF have noted that the "fragmented care" model—where Medicare and Medicaid operate under separate administrative silos—is already a barrier to quality.
Government officials, particularly at the state level, have pointed to the necessity of fiscal discipline in the face of rising healthcare costs. However, critics argue that the "spend-down" mechanism—where individuals must deplete their assets to qualify for Medicaid—creates a perverse incentive that keeps the most vulnerable in a cycle of poverty.
"The administrative burden of navigating two separate, often conflicting systems is a barrier in itself," says one policy researcher. "For an individual with cognitive impairment or a developmental disability, the paperwork required to maintain eligibility for both programs is often a full-time job."
Implications: The Future of Dual Coverage
The implications of the 2025 policy changes are far-reaching. As federal funding for Medicaid is constrained, the following trends are likely to emerge:
1. Fragmentation of Care
If states opt to reduce optional benefits to save money, the continuity of care for the 9 million full-benefit dual-eligibles will be compromised. A reduction in dental or vision coverage, for example, is not merely a loss of a benefit; for a senior with diabetes, poor dental health can lead to systemic infections and increased hospitalizations.
2. Increased Institutionalization
If Medicaid support for home and community-based services is curtailed due to budget cuts, more individuals may be forced into expensive, institutionalized nursing care settings. This would ironically increase costs for the system in the long run, as institutional care is significantly more expensive than home-based support.
3. The "Access Gap"
There is a growing fear that as eligibility thresholds tighten and administrative hurdles increase, the most vulnerable—those with lower literacy, cognitive impairments, or those in rural areas—will simply fall out of the system. This "access gap" could lead to a spike in emergency room visits, as individuals who are no longer able to afford routine care wait until their conditions reach a crisis point.
4. Need for Integrated Care
The data suggests that the current system is not equipped to handle the unique needs of the dual-eligible population. Policy experts are increasingly calling for a "seamless" coverage model that eliminates the dual-enrollment friction. Without such a transition, the health outcomes for the most vulnerable 12 million Americans will continue to be dictated by the administrative interplay of state and federal budgets rather than their actual clinical needs.
In conclusion, the dual-eligible population represents a critical barometer for the health of the American social safety net. As the 2025 budget changes take hold, the intersection of these two programs will remain a focal point for policymakers, advocates, and, most importantly, the millions of families who rely on these services for their day-to-day stability. The challenge remains: how to maintain fiscal sustainability without sacrificing the quality of life for those who have the least.