Editorial Note: Originally published on January 13, 2026, this report has been continuously monitored and updated to reflect the evolving landscape of U.S. foreign health policy. The latest update, as of July 1, 2026, incorporates data from the most recent round of bilateral agreement signings.
Introduction: A New Era of Global Health Engagement
On September 18, 2025, the United States government fundamentally altered its approach to international medical aid with the release of the "America First Global Health Strategy." This strategic pivot moves away from traditional, open-ended development assistance toward a model defined by finite, results-oriented bilateral cooperation agreements. Known as Memorandums of Understanding (MOUs), these documents serve as the blueprints for U.S. engagement in global health through 2030, signaling a clear intent to foster "country ownership" while tapering long-term U.S. financial dependency.
As the U.S. transitions its global health portfolio, the core objective is to cultivate resilient and durable domestic health systems in partner nations. However, the policy comes with a significant condition: as U.S. assistance recedes over the next five years, partner nations are required to demonstrate increased "co-investment," or domestic health spending, to fill the projected funding gaps.

Chronology: The Road to the 2026-2030 Framework
The transition to this new strategy was not sudden, but rather the culmination of a multi-year debate regarding the efficacy of U.S. foreign aid.
- Early 2025: Policy planners within the State Department and USAID began drafting the new "America First" framework, emphasizing sustainability and the need for partner countries to take fiscal responsibility for their health sectors.
- September 18, 2025: The U.S. government officially unveils the "America First Global Health Strategy," codifying the transition toward five-year bilateral MOUs.
- Late 2025: The first wave of agreements is signed with key strategic partners. These initial MOUs set the precedent for the negotiation process, focusing on capacity building and phased financial handovers.
- January 2026: The launch of the inaugural tracker for these agreements, providing the public with transparency regarding the specific financial and programmatic commitments made by participating nations.
- July 2026: The most recent update to the program confirms that while the implementation phase is in its infancy, the framework is being applied across a growing number of diverse geographic regions, testing the resilience of the U.S. model against varying economic realities.
Supporting Data: Visualizing the Shift
To track the progress and the fiscal impact of these MOUs, a comprehensive data-tracking initiative has been established. The tracker aggregates information from State Department press releases, U.S. embassy communications, and declarations from partner Ministries of Health.
Key Analytical Metrics
The data currently available provides a window into the scale of the transition:

- Choropleth Mapping: Maps indicate a wide geographic distribution, though the concentration of agreements remains highest in regions where U.S. health aid has historically been the primary driver of public health infrastructure.
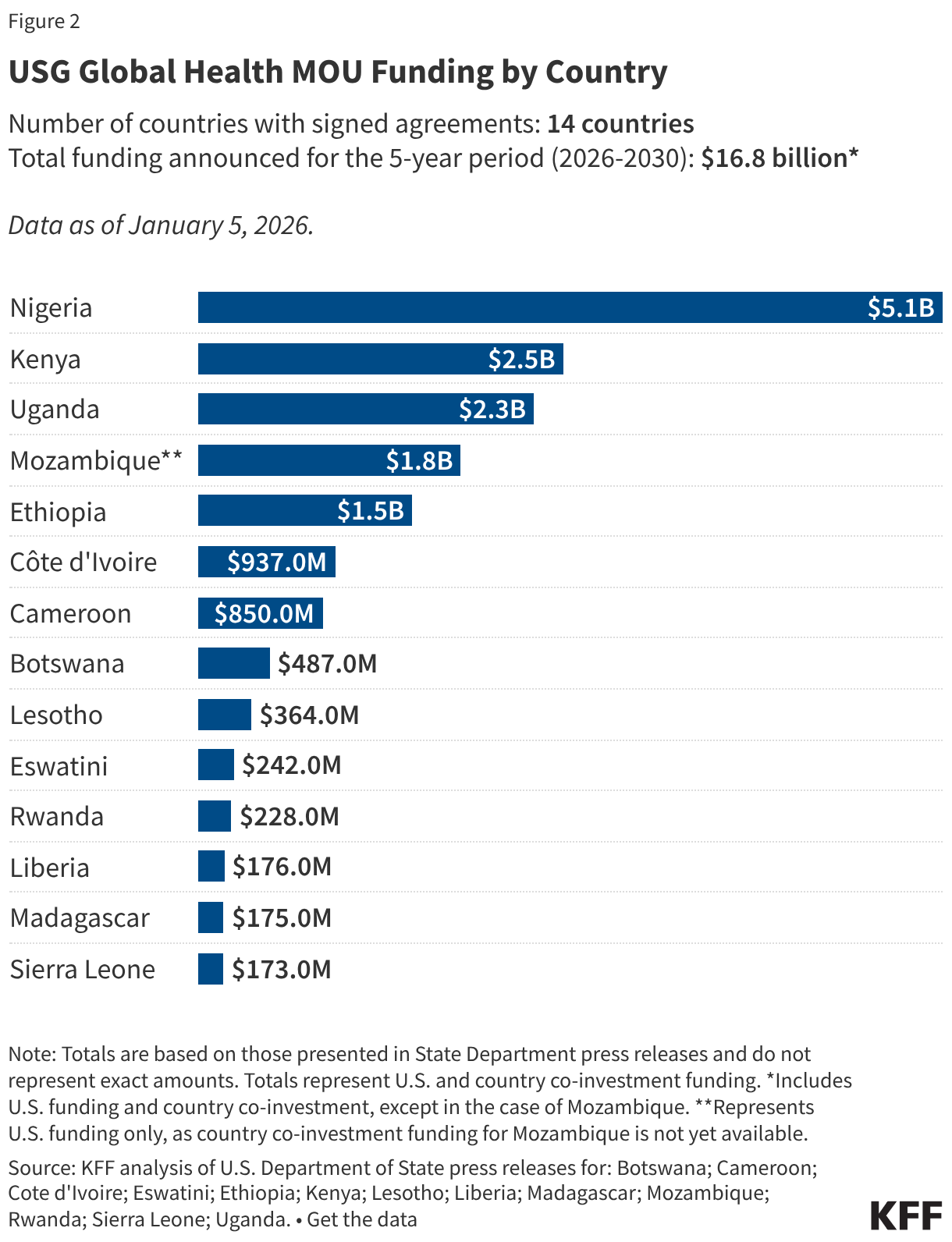
- Funding Trajectories: Bar charts comparing historical U.S. funding levels against the proposed five-year MOU commitments reveal a clear downward trend in U.S. contributions. This is intentionally designed to trigger the "co-financing" requirement.
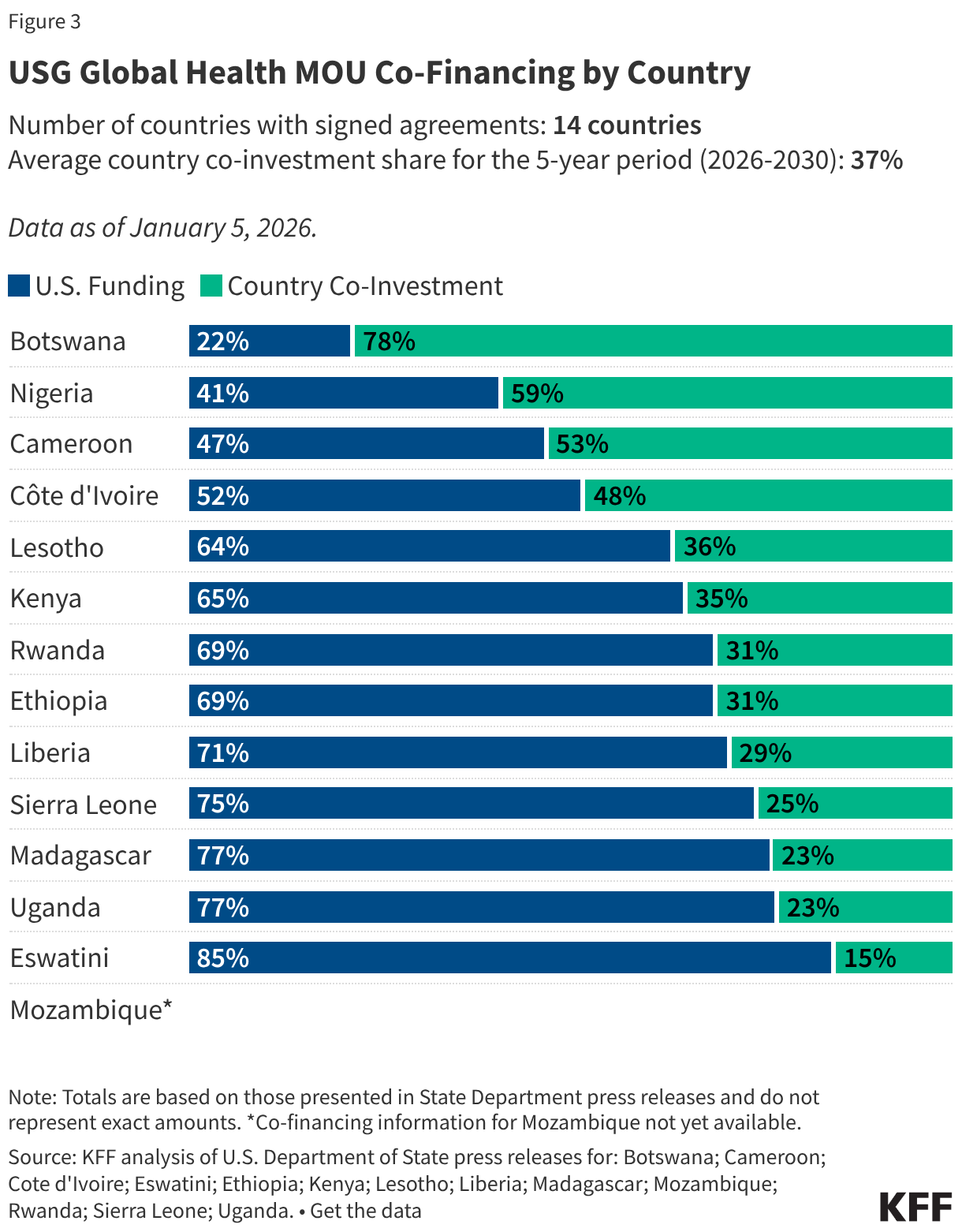
- Co-Financing Shares: Stacked bar charts highlight the specific percentages that partner countries have committed to contribute. This data serves as the primary metric for measuring the success of the "America First" transition.
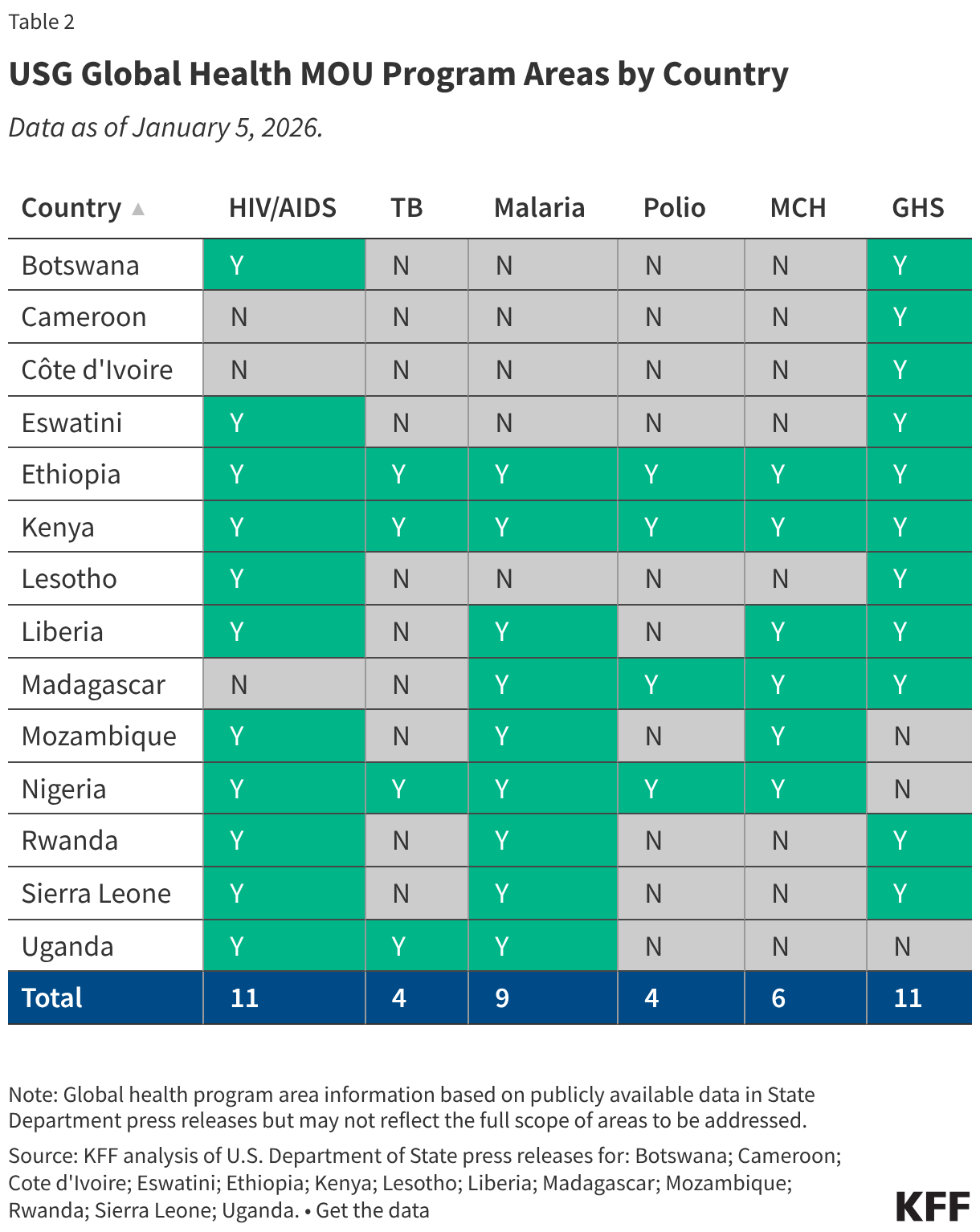
- Programmatic Focus: Tables derived from keyword analysis indicate that while "Global Health Security" (GHS) remains a priority—specifically regarding outbreak preparedness—other legacy programs are being re-evaluated for sustainability.
Methodological Note: Because the text of many MOUs remains proprietary or classified, the tracker relies heavily on public-facing summaries. For countries where the full text is available, calculations reflect the sum of annual commitments. Program areas are categorized based on explicit mentions of health security, disease containment, and outbreak response in official statements.
Official Responses and Stakeholder Perspectives
The reception to the "America First Global Health Strategy" has been bifurcated.
The U.S. Position:
Administration officials argue that the shift is not a retreat from global health, but a move toward "maturity." By mandating domestic co-investment, the U.S. argues it is preventing the "aid trap," where countries remain perpetually reliant on Washington to fund basic immunizations and clinic operations. The goal, according to the State Department, is to ensure that by 2030, these nations possess the sovereign fiscal capacity to manage their own health threats without reliance on external emergency funding.

The Partner Country Perspective:
Ministries of Health in developing nations have expressed a mix of cooperation and anxiety. While many welcome the emphasis on long-term systemic sustainability, there is concern regarding the aggressive timelines. In countries with limited tax bases, the requirement to scale up domestic spending on health while U.S. aid decreases has been described by some health ministers as a "high-stakes fiscal gamble."
Global Health Advocates:
Non-governmental organizations (NGOs) and international health policy analysts have raised concerns regarding the "keyword-limited" nature of these agreements. Critics argue that if an MOU does not explicitly categorize a specific disease or service—such as maternal health or specific chronic care initiatives—under "Health Security," that program might face funding cuts during the transition.
Implications for the Future of Global Health
The implications of this strategy are profound and reach far beyond the next five years.
1. The Resilience Metric
The core test of the "America First" strategy will be the durability of health systems in the face of a crisis. If a country experiences an outbreak of a novel pathogen in 2029, will its domestic systems be strong enough to manage the threat, or will the reduced U.S. presence leave a vacuum that results in a greater global threat?
2. The Shift in Diplomatic Soft Power
Global health has historically been one of the most effective tools of American "soft power." By transforming these relationships from one of donor-recipient to a more transactional, business-like model, the U.S. may be trading influence for fiscal savings. The risk is that other global powers may step into the funding gaps, effectively shifting the diplomatic alliances of these partner nations away from Washington.
3. Sustainability vs. Vulnerability
The emphasis on "long-term country ownership" is theoretically sound—it is the gold standard of development economics. However, the success of this strategy hinges on the economic growth of the partner countries. If the global economy remains volatile, the requirement for increased domestic co-investment may force these governments to choose between funding health systems and servicing national debt.
4. Data Transparency and Accountability
The commitment to provide a public tracker for these MOUs is a significant step toward accountability. As more MOU texts are made public, the international community will be able to perform more granular analyses of how "Global Health Security" is being defined and whether the funding is reaching the most vulnerable populations or being diverted to administrative overhead.
Conclusion: Looking Toward 2030
As we move into the latter half of the 2026-2030 period, the focus will shift from the signing of agreements to their implementation. The U.S. government has set an ambitious course that seeks to rewrite the rules of global health assistance. Whether this strategy creates the "resilient and durable health systems" it promises or exposes gaps in global health security remains the central question of the decade.
The ongoing updates to the MOU tracker will remain the most critical resource for policymakers, researchers, and citizens to monitor this historic transition. As new data becomes available, the narrative of the "America First Global Health Strategy" will continue to evolve, reflecting the real-world outcomes of a policy that is fundamentally redefining the relationship between the world’s most powerful economy and the global health landscape.
For more information on the methodology of this tracker or to access the underlying data sets, please refer to the technical appendix on the State Department’s portal. This report will be updated on a quarterly basis as new bilateral agreements are ratified.