For decades, the KRAS gene—a critical regulator of cellular growth—was considered the "holy grail" of oncology and simultaneously the most elusive. Known as "undruggable" due to its smooth, featureless surface, KRAS mutations drive a significant percentage of human cancers. However, the emergence of the KRAS G12C mutation provided a breakthrough: a small binding groove that allowed for the development of targeted covalent inhibitors.
While first-generation therapies like sotorasib and adagrasib successfully locked the protein in its inactive state, they faced a fundamental biological hurdle: most KRAS G12C proteins in cancer cells remain stubbornly in the active, "on" position. Merck & Co. has now entered the arena with a different philosophy. Instead of pursuing maximum monotherapy potency, the pharmaceutical giant has engineered calderasib as a platform for potent combinations, a strategy that is already yielding impressive clinical signals.
The Strategic Shift: Designing for Synergy
Merck’s approach with calderasib represents a calculated evolution in precision medicine. Jane Healy, vice president and head of oncology early development at Merck Research Laboratories, emphasizes that the molecule was never intended to stand alone as the singular solution to KRAS mutations.
"We didn’t design calderasib to be the most potent KRAS G12C inhibitor on its own," Healy explains. "It was designed to be the most combinable inhibitor."
This distinction is vital. Because KRAS is a central node in numerous cellular signaling pathways, cancer cells often develop resistance by activating bypass tracks. By prioritizing "combinability"—a design feature characterized by high specificity for mutant KRAS and minimized interaction with the wild-type protein—Merck aims to reduce toxicity while maximizing the therapeutic ceiling. This allows the drug to be paired with other agents, such as cetuximab and chemotherapy, without creating a cumulative toxicity profile that would force patients to discontinue treatment.
Chronology of a Breakthrough: From Bench to Bedside
The journey of calderasib is rooted in lessons learned from Merck’s historical success with pembrolizumab.
- The Pre-Clinical Foundation: Researchers focused on overcoming the limitations of early-generation inhibitors that only captured the fraction of KRAS proteins cycling into the inactive state.
- The KANDLELIT-001 Trial: The Phase 1 study served as the primary proving ground for calderasib. It was designed not only to assess safety and objective response rates (ORR) but to pioneer the use of circulating tumor DNA (ctDNA) as a dynamic biomarker.
- The Biomarker-First Strategy: Mirroring the success of the KEYNOTE-158 program, which led to the first tumor-agnostic approval for pembrolizumab, Merck is applying a similar "mutation-over-tissue" strategy to calderasib.
- Future Horizons: With the positive data from the KANDLELIT-001 trial in hand, Merck has initiated the Phase 3 KANDLELIT-012 trial, which will evaluate the triple-therapy regimen (calderasib, cetuximab, and chemotherapy) in first-line colorectal cancer (CRC).
Supporting Data: Validating the Combinability Thesis
The clinical data from the KANDLELIT-001 trial provides the most robust evidence to date that Merck’s design philosophy is sound. The results demonstrate a clear, positive correlation between the intensity of the treatment regimen and the clinical response.
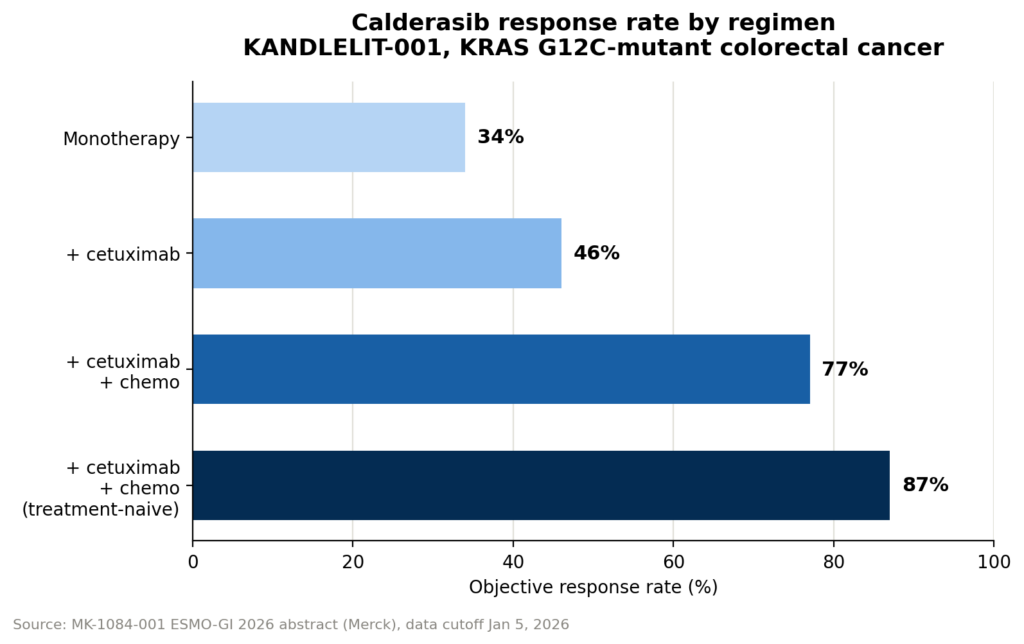
Clinical Response Rates
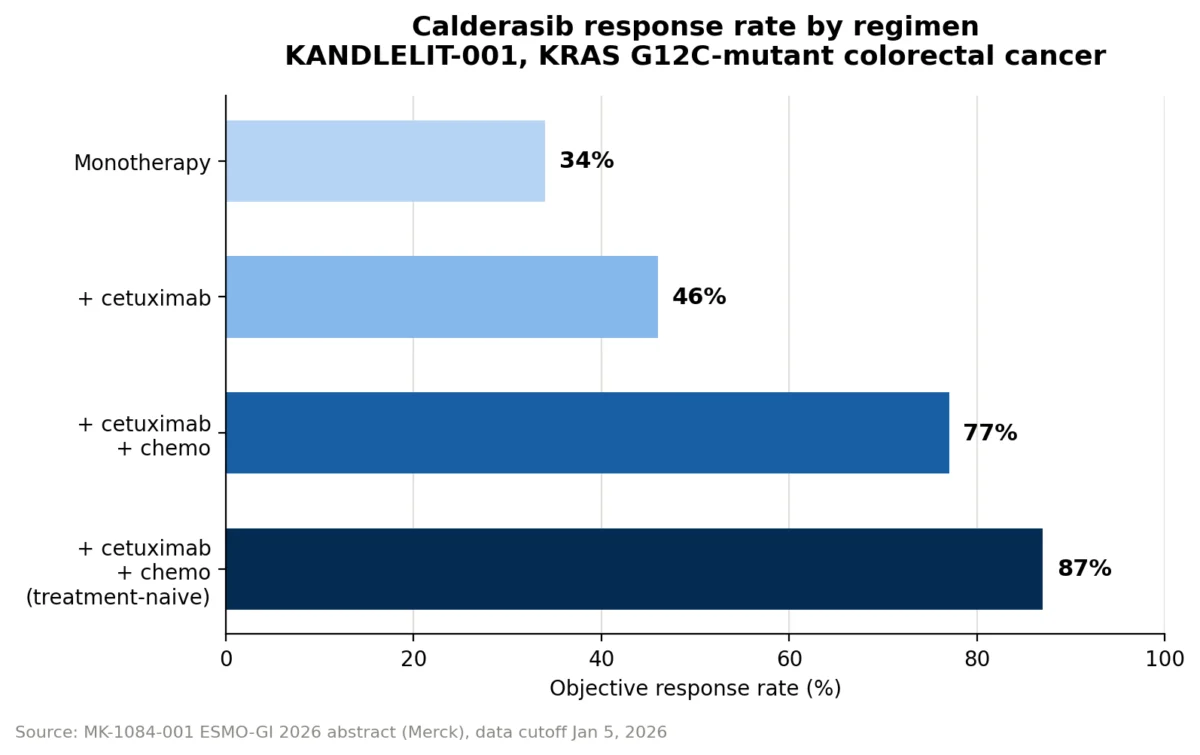
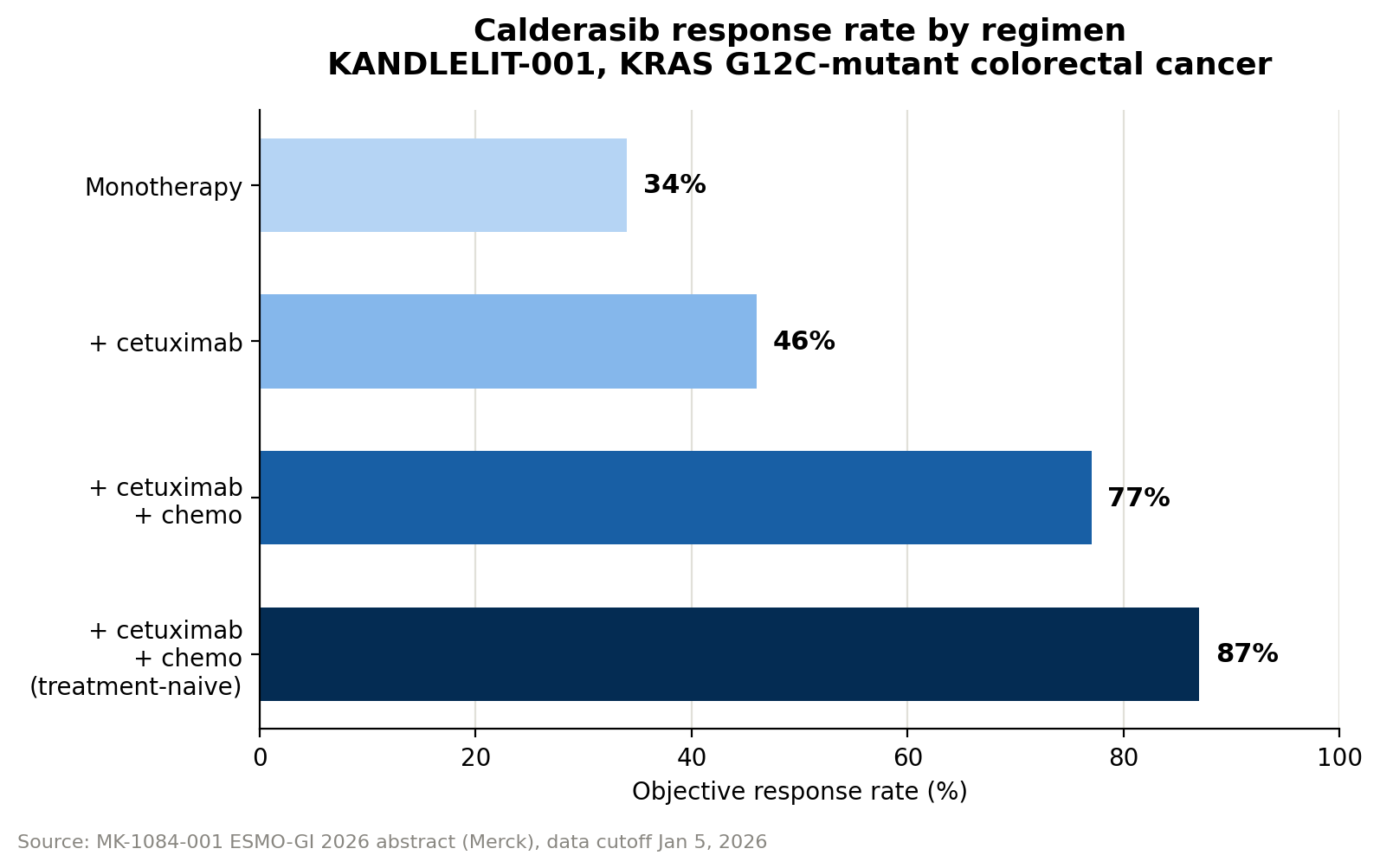
- Monotherapy: Calderasib alone demonstrated an objective response rate (ORR) of 34%.
- Doublet Therapy: When combined with the EGFR inhibitor cetuximab, the ORR increased to 46%.
- Triplet Therapy: The addition of standard chemotherapy boosted the ORR to 77%.
- First-Line Potential: In patients who had not yet received prior systemic therapy, the triplet regimen achieved an remarkable 87% response rate.
Managing Toxicity
While the triplet regimen significantly improves efficacy, it naturally introduces higher toxicity. Grade 3 or 4 drug-related adverse events were observed in:
- 9% of patients on calderasib monotherapy.
- 20% of patients on the doublet.
- 42% of patients on the triplet.
Despite the rise in adverse effects, clinical leadership maintains that the toxicity profile remains manageable and is consistent with the known side effects of the individual components.
Tracking Response via the Blood: The Role of VAF
One of the most innovative aspects of the KANDLELIT-001 study is the reliance on variant allele fraction (VAF)—the proportion of circulating tumor DNA that carries the KRAS G12C mutation.
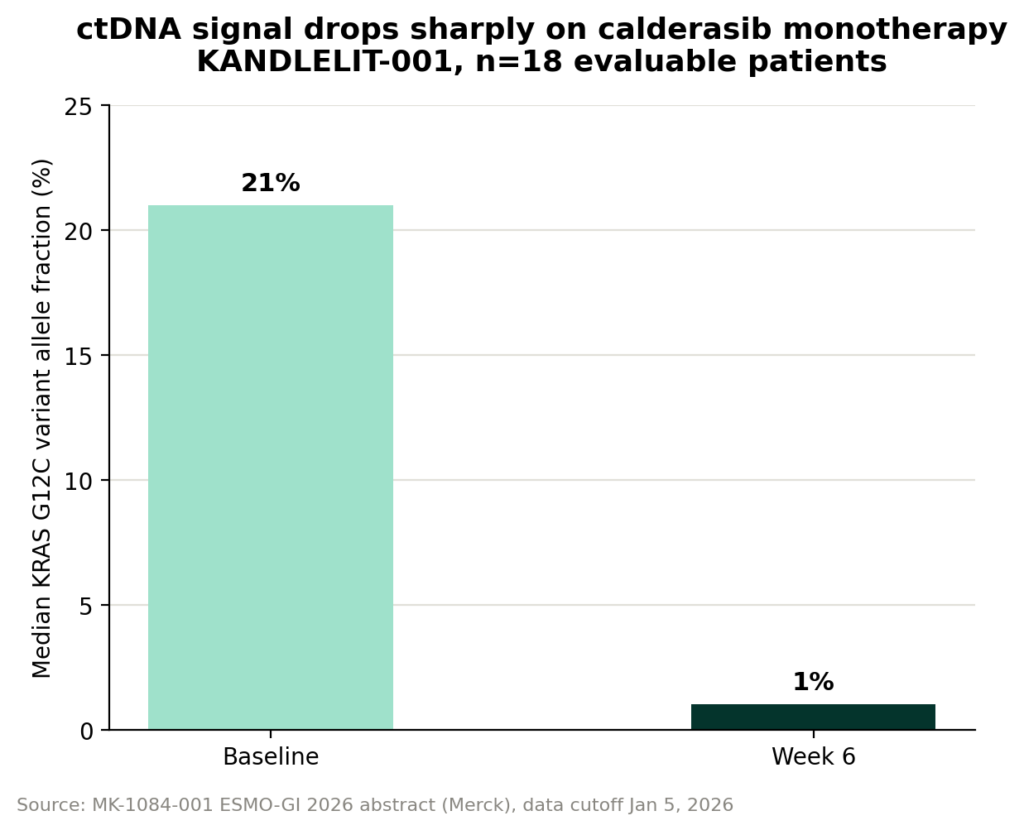
Because ctDNA is shed by tumor cells into the bloodstream, it provides a real-time, non-invasive "liquid biopsy." In the KANDLELIT-001 trial, researchers measured VAF at multiple intervals. The results were compelling: in monotherapy, calderasib reduced VAF by a median of approximately 95%—plummeting from 21% at baseline to 1% by week 6.
"If you track the KRAS G12C variant allele fraction over the course of treatment, it declines, and we can track that across all patients in the study," says Healy. "The reduction in VAF in the blood correlates quite nicely with the responses we’re seeing by imaging."
This biomarker-driven monitoring offers a significant advantage over traditional imaging. While scans are definitive, they are costly, burdensome, and infrequent. VAF monitoring allows for high-frequency checks, potentially identifying resistance or progression long before a tumor becomes visible on a CT or PET scan. However, it is important to note that VAF is a relative measure; it reflects the proportion of mutant DNA relative to total cell-free DNA, meaning it must be interpreted alongside other clinical data.
Implications: The Tumor-Agnostic Paradigm
Merck’s decision to move forward with a pan-tumor, biomarker-driven study for calderasib is a bold validation of the "tumor-agnostic" approach. Having pioneered this with pembrolizumab—first with MSI-High status and later with tumor mutational burden—Merck is now betting that KRAS G12C status is a sufficient marker to guide therapy regardless of whether the cancer originated in the lung, colon, or elsewhere.
Why this matters
- Efficiency: By focusing on the genetic driver rather than the organ of origin, the drug development process can theoretically move faster, capturing efficacy across broader patient populations.
- Standardization: This approach provides a clear path for clinicians. If a patient’s molecular profile shows a KRAS G12C mutation, the treatment decision becomes clearer, reducing the guesswork associated with tissue-specific protocols.
- Durable Development: This is not a one-off regulatory maneuver. By applying the same logic to a second drug nearly a decade after the first, Merck is signaling that the biomarker-first philosophy is now a fundamental pillar of their oncology strategy.
Conclusion: The Road Ahead
The success of calderasib hinges on whether the impressive results from the KANDLELIT-001 trial hold up in larger, randomized Phase 3 environments. If the 87% response rate in first-line patients translates into durable progression-free survival, calderasib could fundamentally alter the standard of care for KRAS-mutated cancers.
As we move toward a future where "cancer" is increasingly defined by its genetic signature rather than its location in the body, Merck’s focus on "combinability" may prove to be the most critical design choice of the decade. While the data is still maturing, the trajectory is clear: by treating the mutation and mastering the combination, the clinical community is finally turning the page on the "undruggable" KRAS protein.
The upcoming results from the KANDLELIT-012 trial will be the final test of this thesis, and the oncology community will be watching closely to see if the promise of these early biomarkers translates into lasting clinical benefit for patients worldwide.