On June 1, 2026, the Centers for Medicare and Medicaid Services (CMS) finalized an interim rule that fundamentally alters the landscape of public health coverage in the United States. Following the passage of the 2025 federal budget reconciliation law, the new mandate requires states to impose "community engagement" or work requirements on certain Medicaid enrollees, specifically those covered under the Affordable Care Act (ACA) expansion or specific waivers.
This policy shift has ignited a firestorm of legal and ethical debate, particularly regarding how states define "medical frailty." As the nation grapples with these changes, the population most vulnerable to these administrative hurdles—individuals living with HIV—finds itself at a critical juncture. The regulation, which ties eligibility to employment or volunteerism, introduces a complex, two-part test for medical exemptions that patient advocates warn could lead to widespread coverage loss, compromising both individual health outcomes and national HIV eradication goals.
Chronology: From Policy Proposal to Federal Litigation
The path to the current crisis began with the 2025 federal budget reconciliation law, which granted states the authority to condition Medicaid eligibility on employment status. While states were historically permitted to seek waivers for such programs, the new federal law effectively mainstreamed these requirements, prompting CMS to provide the necessary regulatory framework.
- June 1, 2026: CMS releases the interim final rule, establishing guidelines for community engagement and defining the "medically frail" exclusion. The rule mandates that an enrollee must not only have a qualifying condition but must also prove that the condition specifically impairs their ability to meet the work requirement.
- June 29, 2026: A coalition of 24 states and two governors files a lawsuit against CMS in the U.S. District Court for the District of Massachusetts. The plaintiffs argue that the "two-part test" for medical frailty is an arbitrary departure from legislative intent and creates an impossible administrative burden.
- Present Day: As the legal battle unfolds, states are scrambling to interpret the rule, with some—like Nebraska—having already attempted to implement restrictive, code-based criteria for exemptions that fail to account for the full clinical reality of chronic diseases like HIV.
Supporting Data: The Medicaid-HIV Nexus
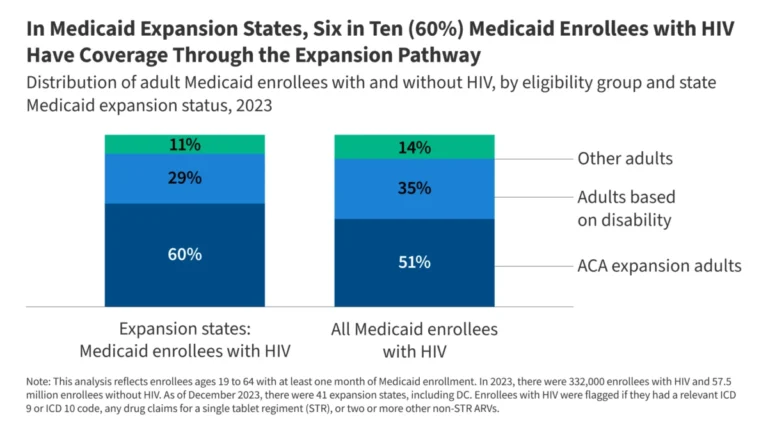
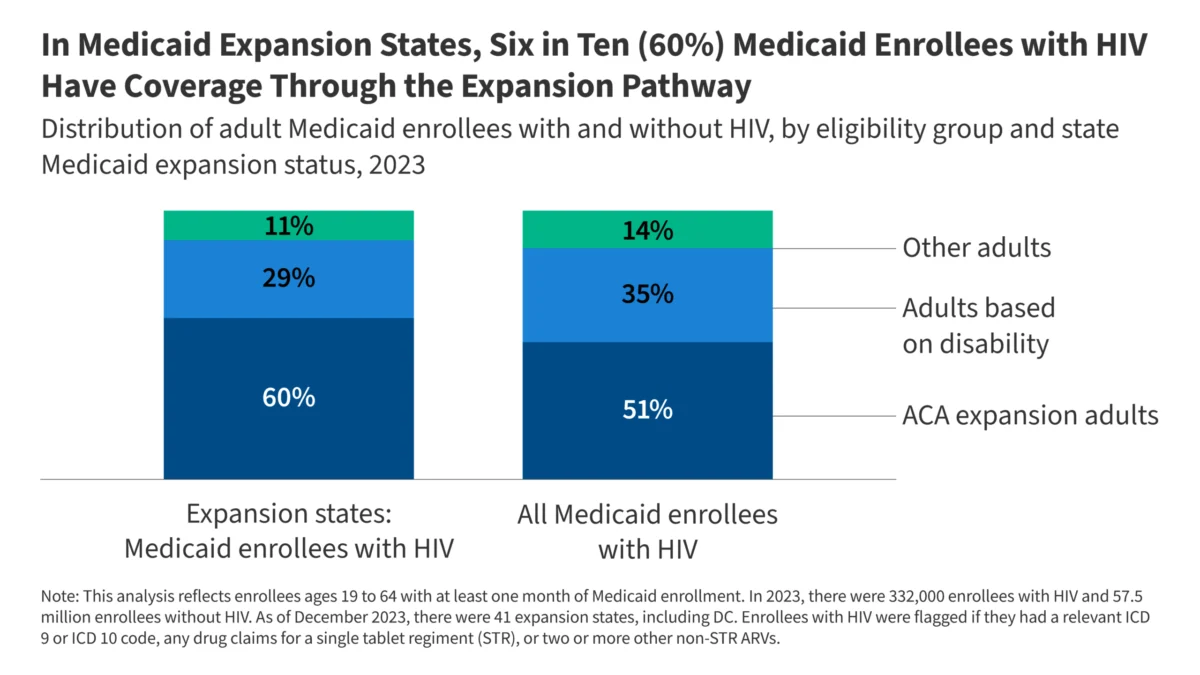
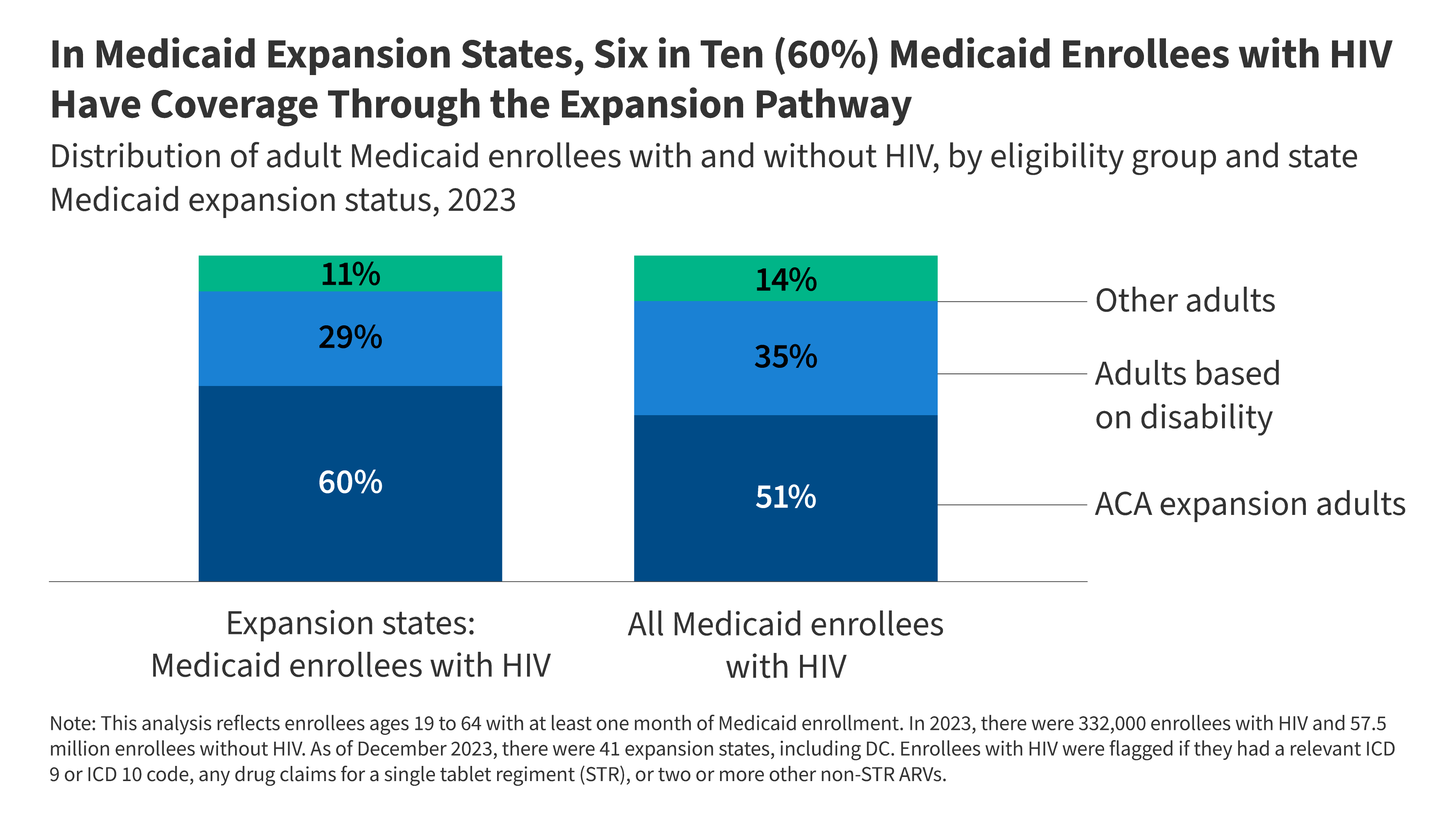
Medicaid has evolved into the bedrock of HIV care in the United States. According to the latest data, nearly half (46%) of all individuals living with HIV in the U.S. rely on Medicaid for their life-saving antiretroviral therapy and primary care.
The reliance on this program is even more pronounced in states that chose to expand Medicaid under the ACA. In these jurisdictions, 60% of adults under 65 living with HIV utilize the expansion pathway for coverage. Before the expansion, many individuals with HIV were forced to wait until their condition advanced to the point of permanent disability to qualify for federal assistance. The current work requirements threaten to return these patients to a state of medical limbo, where they must either maintain perfect employment or navigate an increasingly complex bureaucracy to retain coverage.
Furthermore, the clinical profile of this population necessitates stability. Approximately 73% of Medicaid-enrolled individuals with HIV manage at least one additional chronic condition, such as hypertension or diabetes. Additionally, 23% have a substance use disorder (SUD) diagnosis, and 36% have a diagnosed mental health condition. With 50% of the population reporting some form of functional disability—ranging from mobility issues to stage III AIDS—the "ability to work" is not merely a matter of effort, but a matter of severe physical and mental capacity.
The Two-Part Test: A Barrier to Care
The core of the controversy lies in the CMS definition of "medical frailty." Under the new rule, having a diagnosis like HIV is no longer sufficient to automatically qualify for an exemption. Instead, enrollees must demonstrate that their HIV diagnosis—or any other qualifying condition—significantly impairs their ability to perform the work required by the state.
This creates a "double burden of proof." First, the patient must be diagnosed with a condition deemed "serious or complex." While CMS acknowledges HIV as a potential qualifying condition, it caveats this by stating that the exemption is "less likely to be the case if the acuity of their condition is not severe." This language creates a dangerous precedent: patients who are successfully managing their HIV through medication—and thus remain healthy enough to work—could be penalized for their own success. If they lose Medicaid, their health will inevitably decline, leading to the very "severity" the rule purportedly seeks to exempt.
The Administrative Maze
States are now required to maintain "auditable lists" of diagnosis codes to identify the medically frail. However, as seen in Nebraska’s early implementation attempts, these lists are often dangerously incomplete. By failing to include the full spectrum of ICD-10 codes associated with HIV, states risk automatically disqualifying thousands of patients from the exemption process before they even have a chance to appeal.
Official Responses and Legal Arguments
The plaintiffs in the Massachusetts lawsuit argue that the two-part test is a gross overreach of the original reconciliation law. Their core contention is that the statute was designed to protect the vulnerable, not to force them into a clinical audit.
"People with disabilities, patients in the middle of cancer treatment, or those struggling with other serious or complex health conditions shouldn’t be at risk of losing the care that helps maintain their health," the complaint asserts. The states argue that forcing patients to prove that their specific condition limits their ability to work turns clinicians into "eligibility gatekeepers," a role that strains the provider-patient relationship and diverts time from actual patient care.
CMS, conversely, maintains that the rule is a necessary exercise of federal oversight to ensure consistent application of the law across state lines. They argue that the inclusion of various clinicians—including clinical social workers—in the verification process provides enough flexibility for providers to advocate for their patients.
Implications for Public Health and the HIV Epidemic
The potential fallout of these requirements extends far beyond the individual patient. The "churn" of patients moving on and off Medicaid due to reporting failures and administrative red tape poses a significant threat to the nation’s "Ending the HIV Epidemic" (EHE) initiative.
The Risk of Treatment Interruption
For those living with HIV, adherence to antiretroviral therapy (ART) is the single most important factor in preventing viral transmission. Current research indicates that four in ten new HIV infections are linked to individuals who are aware of their status but are not currently in care. If work requirements lead to even temporary gaps in insurance coverage, patients may be unable to afford their medication, leading to viral load rebound, increased morbidity, and the potential for drug-resistant HIV strains to emerge.
Strain on the Ryan White Program
When individuals lose Medicaid, they often turn to the federal Ryan White Program as a safety net. However, the Ryan White system is currently operating under severe budget constraints. Expecting these programs to absorb the influx of patients displaced by Medicaid work requirements is, according to public health experts, a recipe for systemic collapse.
Conclusion: A Delicate Balance
The CMS rule on Medicaid community engagement attempts to balance fiscal responsibility with healthcare access, but for the HIV community, the math does not add up. By imposing a stringent, two-part definition of medical frailty, the rule creates a high-stakes environment where the most vulnerable must navigate complex administrative requirements just to maintain access to life-saving treatment.
As the legal challenge in Massachusetts proceeds, the healthcare community remains on high alert. The outcome of this case will not only determine the future of Medicaid work requirements but will also signal the nation’s commitment to the health and dignity of its most vulnerable citizens. Whether through judicial intervention or further administrative refinement, a clear path is needed—one that recognizes that for people living with HIV, access to medical care is not a reward for employment, but a fundamental necessity for survival.