For millions of older Americans, the promise of Medicare Advantage (MA) is one of integrated, managed care—a private-sector alternative to the traditional federal program designed to offer efficiency and enhanced benefits. However, a growing body of evidence, bolstered by recent investigations from the Office of Inspector General (OIG), suggests that the reality for many beneficiaries is a complex, high-stakes gauntlet of administrative barriers. At the center of this controversy is "prior authorization," a process that has evolved from a cost-control mechanism into a significant hurdle for patients seeking the most critical forms of post-acute care.
The Core Conflict: Efficiency vs. Access
Prior authorization is, in theory, a tool for medical necessity. Insurers argue that it protects the system from "low-value" care and helps contain the ballooning costs of the healthcare sector. Yet, public sentiment has soured significantly. According to recent KFF polling, seven in ten insured adults now view prior authorization as a significant burden, a sentiment that is increasingly backed by federal data.
With more than half of all Medicare beneficiaries now enrolled in private Medicare Advantage plans, the stakes have never been higher. When these plans deny coverage for hospital stays, rehabilitation, or nursing care, the consequences are not merely bureaucratic—they are deeply personal, often impacting the most vulnerable patients in the most fragile states of health.
A Chronology of Increasing Scrutiny
The scrutiny surrounding Medicare Advantage prior authorization is not a recent development, but rather the culmination of years of mounting concern from regulators, lawmakers, and patient advocates.
- 2019–2022: A multi-year investigation by the Senate Permanent Subcommittee on Investigations (PSI) revealed that the nation’s largest Medicare Advantage insurers were disproportionately denying prior authorization requests for post-acute care. This set the stage for a broader federal inquiry.
- Summer 2024: Faced with mounting public pressure, several major private insurers made public pledges to streamline and "improve" their prior authorization processes. However, these voluntary commitments have been met with skepticism by policy analysts who point to a lack of measurable, transparent data.
- Late 2024–2025: The OIG released two landmark reports documenting the staggering denial rates for specific, high-cost services. These reports solidified the argument that systemic issues, rather than isolated administrative errors, were driving the current crisis.
- 2027 and Beyond: The Centers for Medicare & Medicaid Services (CMS) has initiated a pilot program to collect granular, service-level data on denials. The industry anticipates that mandatory, standardized reporting will become the new federal requirement by 2027, potentially ending the "black box" era of managed care oversight.
Supporting Data: The High Cost of Denial
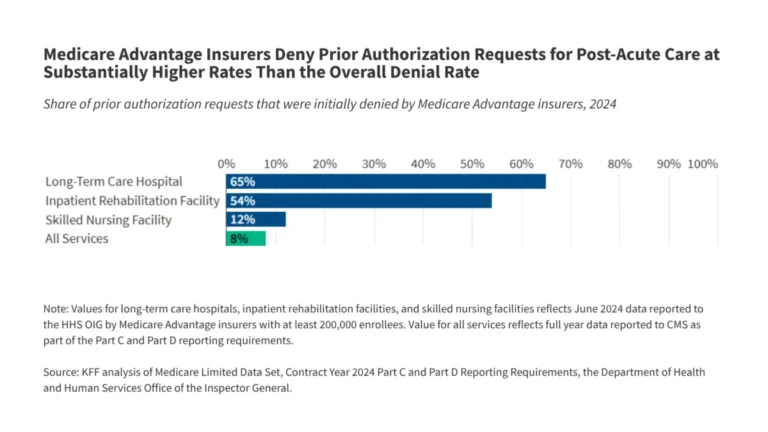
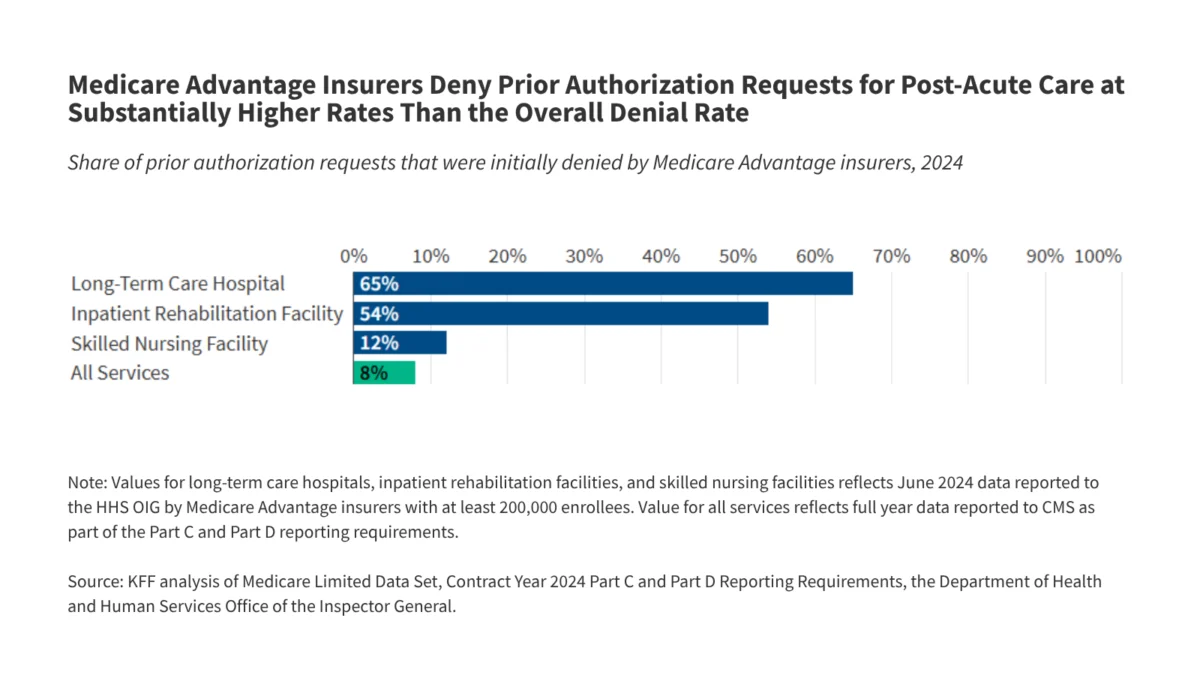
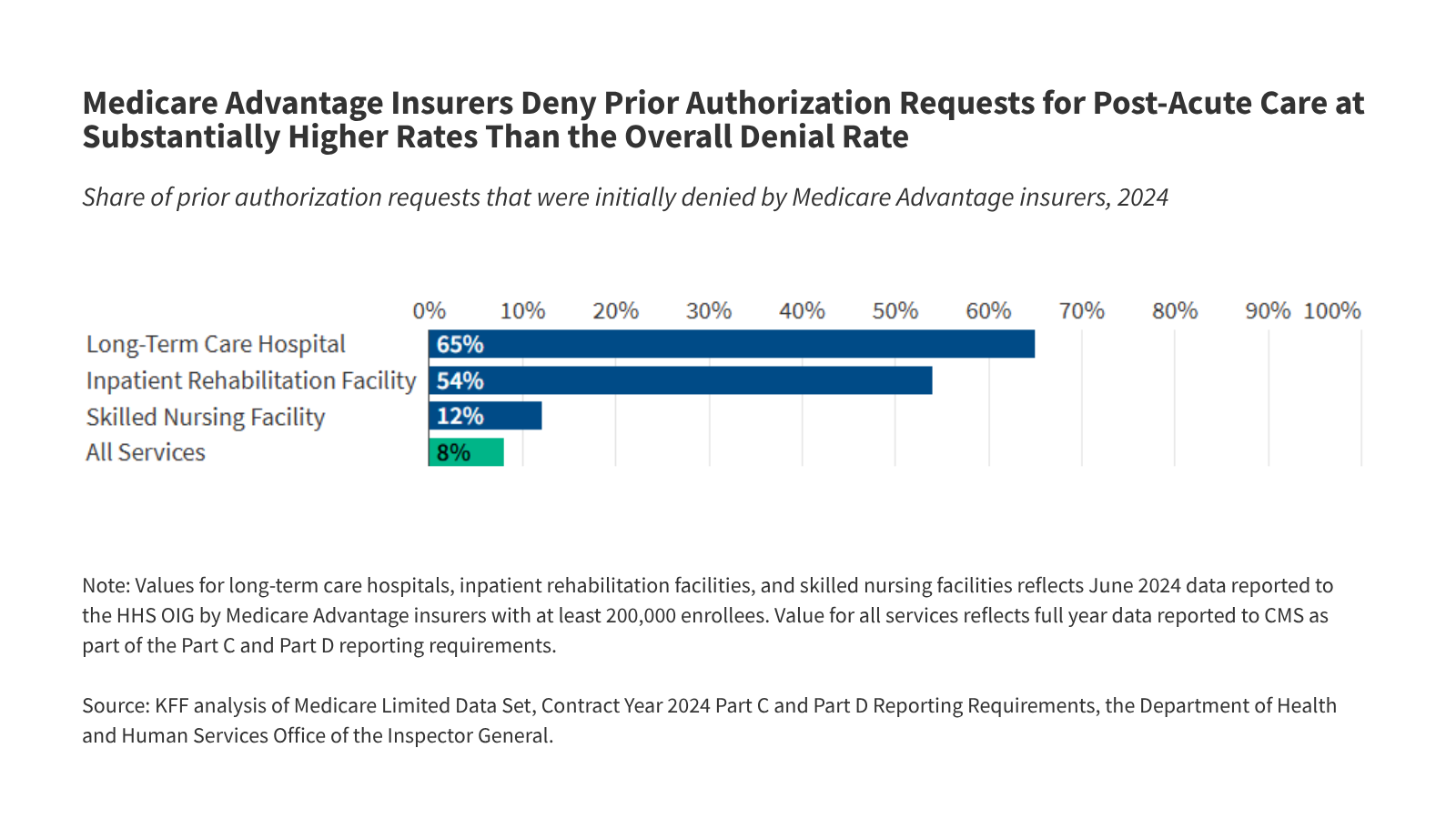
The OIG’s recent findings are striking, particularly when compared to the baseline denial rates for all Medicare Advantage services. While the overall denial rate for all services in the Medicare Advantage landscape hovers at approximately 8%, the rates for post-acute care are exponentially higher.
The OIG documented that insurers deny 65% of requests for stays in long-term care hospitals (LTCHs) and 54% of requests for stays in inpatient rehabilitation facilities (IRFs). Even for skilled nursing facilities (SNFs)—the most common post-acute setting—the denial rate sits at 12%.
To understand the financial weight behind these numbers, one must look at the cost of the care being denied. According to the Medicare Payment Advisory Commission (MedPAC), the average Medicare payment in 2023 for an LTCH stay was $43,000. An IRF stay costs roughly $24,000, while a SNF stay averages $16,000. Because insurers are incentivized to control these specific high-cost expenditures, they have turned to rigorous prior authorization as a primary fiscal lever.
Perhaps most alarming is the data regarding appeals. When a patient or their physician challenges a denial, the results suggest that many initial decisions were likely incorrect. For SNF admissions, 95% of appealed denials were overturned. For IRFs, 43% were overturned, and for LTCHs, 36% were overturned. This pattern suggests a "deny-first" mentality that places the onus of proof on patients who are often too ill to navigate the complex appeals process.
Implications for Patient Health and Financial Stability
The implications of these denials extend far beyond the balance sheet. For a patient recovering from a stroke, a traumatic brain injury, or a severe respiratory condition, time is the most critical variable in recovery. The OIG found that an initial denial of a prior authorization request results in an average delay of five to six days of care.
For an elderly patient in a delicate condition, these six days can lead to muscle atrophy, loss of rehabilitation progress, or, in some cases, a decline that prevents them from ever reaching their pre-injury level of function. Furthermore, the financial impact is acute. Many Medicare Advantage plans include daily cost-sharing requirements for hospital stays. Delays caused by administrative back-and-forth can extend the total duration of a patient’s health crisis, thereby increasing their out-of-pocket costs at a time when they are least able to afford them.
There is also a systemic "game" being played. If an insurer denies a claim, they know that only a fraction of patients will have the energy or the medical advocacy to file an appeal. If an insurer expects that 80% of patients will simply accept the denial, the initial decision becomes a profitable fiscal strategy, even if it is medically inappropriate. If the appeal does reach the stage of an Independent Review Entity (IRE), the insurer risks a negative impact on their "Star Ratings," but many believe this risk is currently outweighed by the immediate savings achieved through initial denials.
Official Responses and the Path to Transparency
The lack of transparency remains the most significant hurdle to reform. Because Medicare Advantage plans have historically not been required to report detailed, service-level denial data, regulators have been flying blind.
The Biden-Harris administration and CMS have begun to move the needle. By introducing the new pilot program for data collection, CMS is signaling that the era of opacity is ending. However, the timeline remains a point of contention. While policy experts applaud the move toward 2027, they warn that the current lack of data makes it impossible to hold insurers accountable for the pledges they made last year.
There is also the question of technology. The CMS Innovation Center is currently testing a "Wiser" model, which employs Artificial Intelligence to automate and streamline prior authorization in traditional Medicare. Proponents hope that by digitizing the process, human bias and "slow-walking" tactics can be eliminated. However, critics argue that without robust, independent oversight, AI tools could simply automate the same denial behaviors that are currently causing such distress.
Conclusion: The Search for a Balanced System
The core mission of the Medicare Advantage program is to provide high-quality, efficient care to the aging population. Yet, the evidence suggests that the balance between cost-containment and patient access has tilted dangerously toward the former.
The current system of prior authorization, as it is being deployed in the post-acute sector, is failing to serve the very people it was intended to protect. When 95% of appealed SNF denials are overturned, it is not evidence of a "rigorous" system; it is evidence of a broken one. As the nation approaches the 2027 deadline for mandatory data reporting, the pressure will continue to mount on private insurers to prove that their cost-saving measures do not come at the expense of patient outcomes.
Ultimately, the goal for policymakers must be to ensure that when an elderly patient leaves a hospital, the decision of where they go next is determined by their doctor’s medical expertise—not by an insurance company’s algorithm. Until that balance is restored, the "burden" of prior authorization will remain one of the most pressing challenges in American healthcare.