In the modern clinical landscape, the distance between a "hunch" and a "scientific finding" is measured by the rigor of statistical methodology. For clinicians operating at the bedside, patterns in patient health often seem intuitive—a physician might notice an uptick in bone fractures among a specific cohort of patients taking a particular class of weight-loss medication. When they run the numbers on their own patient records, the data often appear to confirm these suspicions.
However, Brigham Hyde, co-founder of Atropos Health, warns that these initial confirmations are often illusions. "Often a clinician at the point of care will come to us with a hunch—‘I’ve seen a bunch of these patients, I think this might be going on’—and when you run the unmatched analysis, without statistical balancing, it can appear to confirm that hunch. It’s sort of the anecdote becoming the data point," Hyde explains.
The danger lies in the inherent bias of observational data. Without accounting for confounding variables, an analysis may simply be reflecting the physician’s specific patient mix rather than a true biological phenomenon. As real-world evidence (RWE) becomes a cornerstone for regulatory approvals, formulary decision-making, and label-expansion discussions, the distinction between "matched" and "unmatched" studies has evolved from a technical nuance into a fundamental requirement for scientific integrity.
The Evolution of Observational Research: From Anecdote to Insight
The history of clinical research has long been dominated by the gold standard of Randomized Controlled Trials (RCTs). However, as the cost of these trials skyrockets and the complexity of chronic disease management grows, the medical community has increasingly turned to RWE. This approach utilizes vast troves of electronic health records (EHRs) to generate insights that RCTs may take years to uncover.
The challenge, however, is that patients in the "real world" are not assigned to treatments randomly. A patient who receives a surgery for obesity is fundamentally different from a patient prescribed a GLP-1 receptor agonist. If researchers simply compare the outcomes of these two groups, they are not measuring the efficacy of the drug—they are measuring the differences in the baseline health, socioeconomic status, and comorbidities of the individuals who chose those respective treatments.
This is where the methodology of "statistical balancing" becomes critical. By employing techniques such as propensity score matching, researchers can create synthetic cohorts that resemble one another across a spectrum of clinical characteristics, effectively isolating the impact of a single variable, such as a specific medication.
Chronology of a Breakthrough: The Semaglutide Bone Study
A recent study presented at the Endocrine Society’s ENDO 2026 meeting serves as a definitive case study in the necessity of these methodologies. The research, led by Dr. Sun Kim of Stanford University and her colleague Jairo Noreña, began with an observation regarding the fracture risk associated with GLP-1 agonists.
The Initial Inquiry
The team initially identified an apparent lower fracture incidence in patients taking semaglutide compared to those who had undergone sleeve gastrectomy. While the result was intriguing, Dr. Kim remained skeptical. She hypothesized that the finding was not necessarily a reflection of the drug’s protective properties, but rather a byproduct of the significant weight loss achieved through surgery, which carries its own physiological consequences.
Refinement and Methodology
Recognizing the potential for bias, the team pivoted. Instead of comparing a pharmaceutical intervention to a surgical one—which introduces massive confounding variables—they chose to compare semaglutide against other weight-loss agents. Under the leadership of researcher J.N. Velasquez, the team utilized the Atropos Health platform to analyze a robust dataset covering approximately 60,000 patients with type 2 diabetes.
Controlling for Confounders
To ensure the comparison was "apples to apples," the team applied rigorous propensity score matching. They controlled for variables such as age, gender, ethnicity, and a comprehensive comorbidity score. As Hyde notes, "You don’t want a fracture difference to show up simply because everyone in one arm happens to be young and healthy and everyone in the other arm is old and sick."
Furthermore, to address the weight-loss factor directly, the team performed a subgroup analysis of patients who had BMI data recorded both before and after the treatment. This allowed the researchers to isolate the fracture risk even in patients who experienced significant weight reduction.
Supporting Data: The Findings of the 2026 Analysis
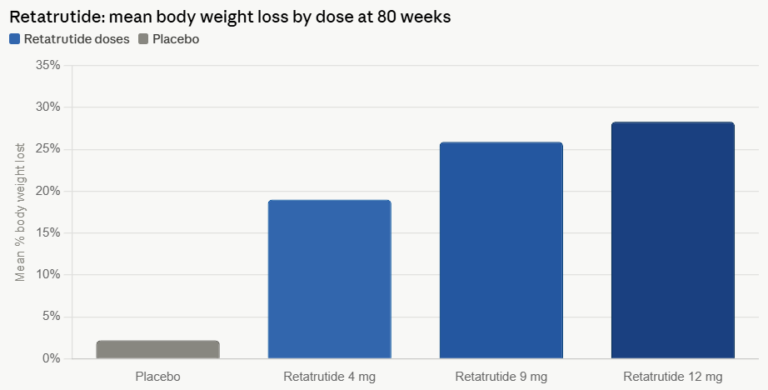
The final data, presented in June 2026, provided a clear, statistically sound answer that contradicted the initial concerns about fracture risk. The study revealed that semaglutide was not associated with an increased risk of bone fractures. In fact, compared to alternative weight-loss therapies, semaglutide was linked to a 15% lower risk of bone fractures.
This finding is significant because it accounts for the potential confounding effects of weight loss. Even when semaglutide patients lost more weight than those on other therapies, their bone health metrics remained stable or improved relative to the control group. The use of propensity score matching provided the researchers—and the endocrinology community—with the confidence to conclude that the protective effect was likely tied to the medication itself rather than the patient population’s baseline health.
Official Responses and the Need for Transparency
For stakeholders—including pharmaceutical sponsors, healthcare providers, and regulatory reviewers—the study highlights a shift in how RWE should be evaluated. Dr. Kim and Brigham Hyde argue that the "topline finding" is no longer enough. Instead, the industry must demand transparency in the methodology behind the data.
The Importance of Balance Tables
Hyde emphasizes the role of the "balance table," a diagnostic tool that explicitly shows how closely the matched groups align on key clinical markers. If a researcher claims to have "matched" two groups, the balance table should provide the numerical proof of that alignment.
"The other essential piece is transparency: you can see the balance tables, how confounding was evaluated, and use that to interpret and build confidence in the results," says Hyde. For any entity reviewing RWE, the first questions should always be:
- Was systematic matching applied?
- Are the matched groups actually balanced on critical comorbidities?
- Is the underlying data visible for audit?
When these questions are ignored, the resulting evidence is fragile. When they are answered with documented rigor, the evidence becomes a powerful tool for informed clinical decision-making.
Implications for the Future of Medicine
The implications of this study extend far beyond the specific findings regarding semaglutide. As we move toward an era of personalized and data-driven medicine, the ability to generate evidence at scale is paramount. We cannot realistically run a randomized controlled trial for every single clinical question; the costs are too high, and the patient population requirements would be impossible to meet in a timely manner.
The Scalability of Real-World Evidence
Real-world data is the only viable path forward for generating evidence at scale. However, the "success" of this path is contingent upon the methodology employed. By adopting the standards seen in the Stanford study—propensity score matching, rigorous control of confounding variables, and total transparency—the medical community can transform observational data into a reliable substitute for traditional trials in appropriate contexts.
Bridging the Gap
For clinicians, the takeaway is clear: personal observations and "hunches" are the starting point of science, not the end. The integration of clinical experience with advanced data analytics platforms like those provided by Atropos Health allows physicians to bridge the gap between their daily observations and the broader truth hidden within population-level data.
As regulatory bodies continue to refine their frameworks for accepting RWE, the focus will undoubtedly remain on the quality of the statistical "plumbing." The semaglutide bone study stands as a model for this evolution, demonstrating that when the data is handled with the right methodology, real-world evidence can be as trustworthy as it is transformative. The days of accepting observational data at face value are ending; the era of verifying the "match" has arrived.