In the landscape of American healthcare, the Medicare Advantage (MA) program has become a dominant force, covering more than half of all Medicare-eligible Americans. Yet, beneath the surface of this private-sector alternative to traditional Medicare lies a complex and increasingly contentious financial mechanism: "risk adjustment." At its heart, this mechanism is intended to ensure that private insurers are compensated fairly for the health status of their enrollees. However, a growing body of evidence suggests that the very tools designed to ensure fairness have created a systemic distortion—a phenomenon known as "coding intensity"—that is costing the federal government tens of billions of dollars annually.
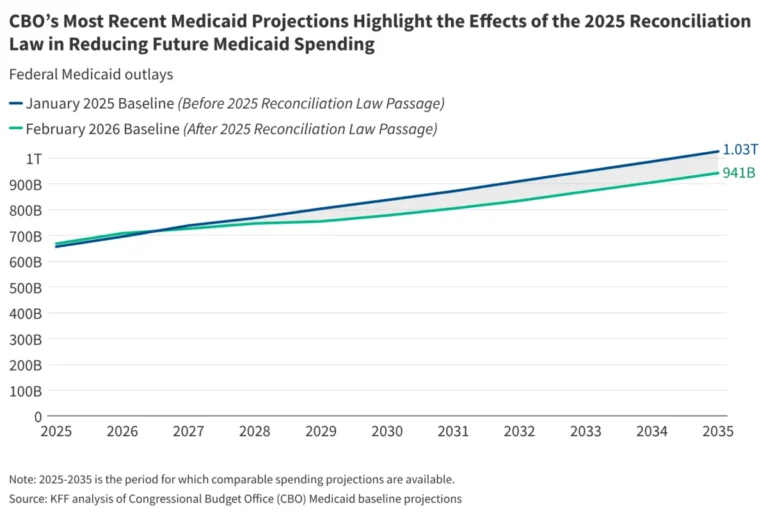
As of 2026, the Medicare Payment Advisory Commission (MedPAC) estimates that total payments to Medicare Advantage plans will exceed what traditional Medicare would have spent for the same beneficiaries by $76 billion. Of that staggering sum, $28 billion is directly attributed to the practice of coding intensity.
The Mechanics of Risk Adjustment: A Financial Incentive
The premise of Medicare Advantage is straightforward: the federal government pays private plans a capitated amount for each enrollee. To prevent insurers from "cherry-picking" only the healthiest patients, the Centers for Medicare & Medicaid Services (CMS) uses a risk adjustment model. Under this system, insurers submit diagnosis codes to CMS. If a patient is identified as having a chronic or complex health condition, the insurer receives a higher payment, reflecting the expected increase in healthcare utilization.
In theory, this is a safeguard for equity. In practice, it creates a massive financial incentive for insurers to maximize the number of diagnosis codes reported for every patient. In the world of "coding," more is better. Every additional diagnosis code—from diabetes to obesity—can act as a lever that increases the federal payment to the plan.
This incentive structure is fundamentally different from traditional Medicare. In the traditional system, providers code only what is necessary to support the services delivered. There is no incentive to inflate the documentation of a patient’s conditions because the payment structure does not rely on those codes to set a capitated rate. This discrepancy leads to the "coding intensity" gap: Medicare Advantage enrollees appear significantly sicker than their traditional Medicare counterparts, even when their clinical realities are identical.
A Chronology of Regulatory Reform
The tension between the need for accurate payments and the reality of aggressive coding has spurred a decade of policy evolution.
- Pre-2024: CMS relied on older risk adjustment models (such as V24). During this period, coding intensity grew unchecked, with studies suggesting that the "uncorrected" impact of coding on payments reached as high as 10% by 2022.
- 2024–2026 (The V28 Transition): Recognizing the systemic distortion, CMS began a phased rollout of the V28 risk adjustment model. This update overhauled how certain conditions were incorporated into payment calculations, effectively pruning the list of diagnosis codes that trigger additional federal funds.
- 2027 Rate Notice: In its most recent regulatory maneuver, CMS finalized a policy to exclude diagnosis codes derived from "unlinked" chart reviews. Previously, insurers would perform internal chart audits to retroactively add diagnosis codes for conditions that were never actually treated during a physician encounter. By removing these "unlinked" codes, CMS aims to curb the practice of artificial inflation.
Supporting Data: The Magnitude of the Distortion
The financial data provided by independent analysts and MedPAC paints a clear picture of the scale of this issue. The $76 billion gap between MA and traditional Medicare spending is composed of two primary drivers: coding intensity ($28 billion) and "favorable selection" ($57 billion).
The Coding Intensity Example: The Case of "Mr. Smith"
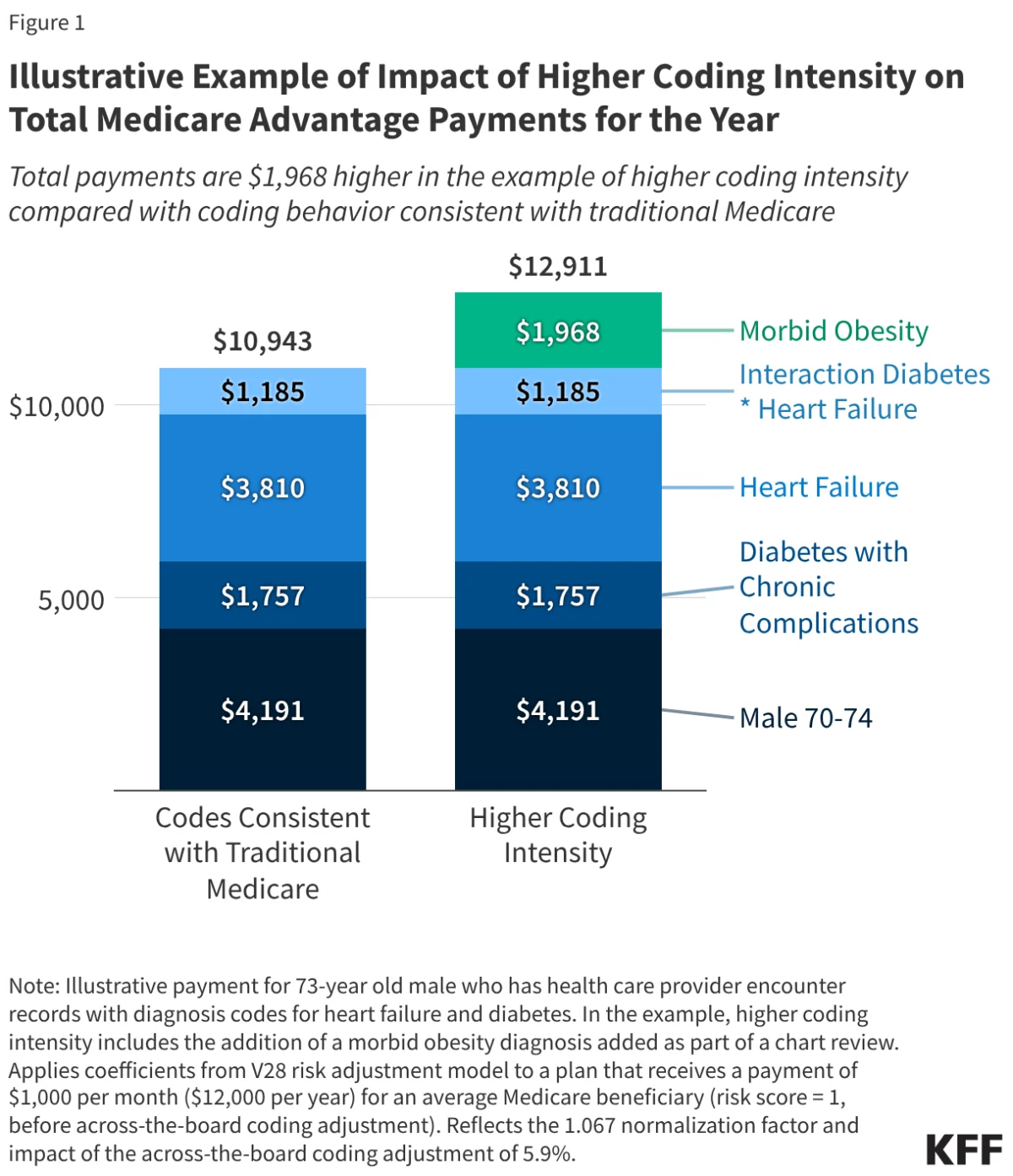
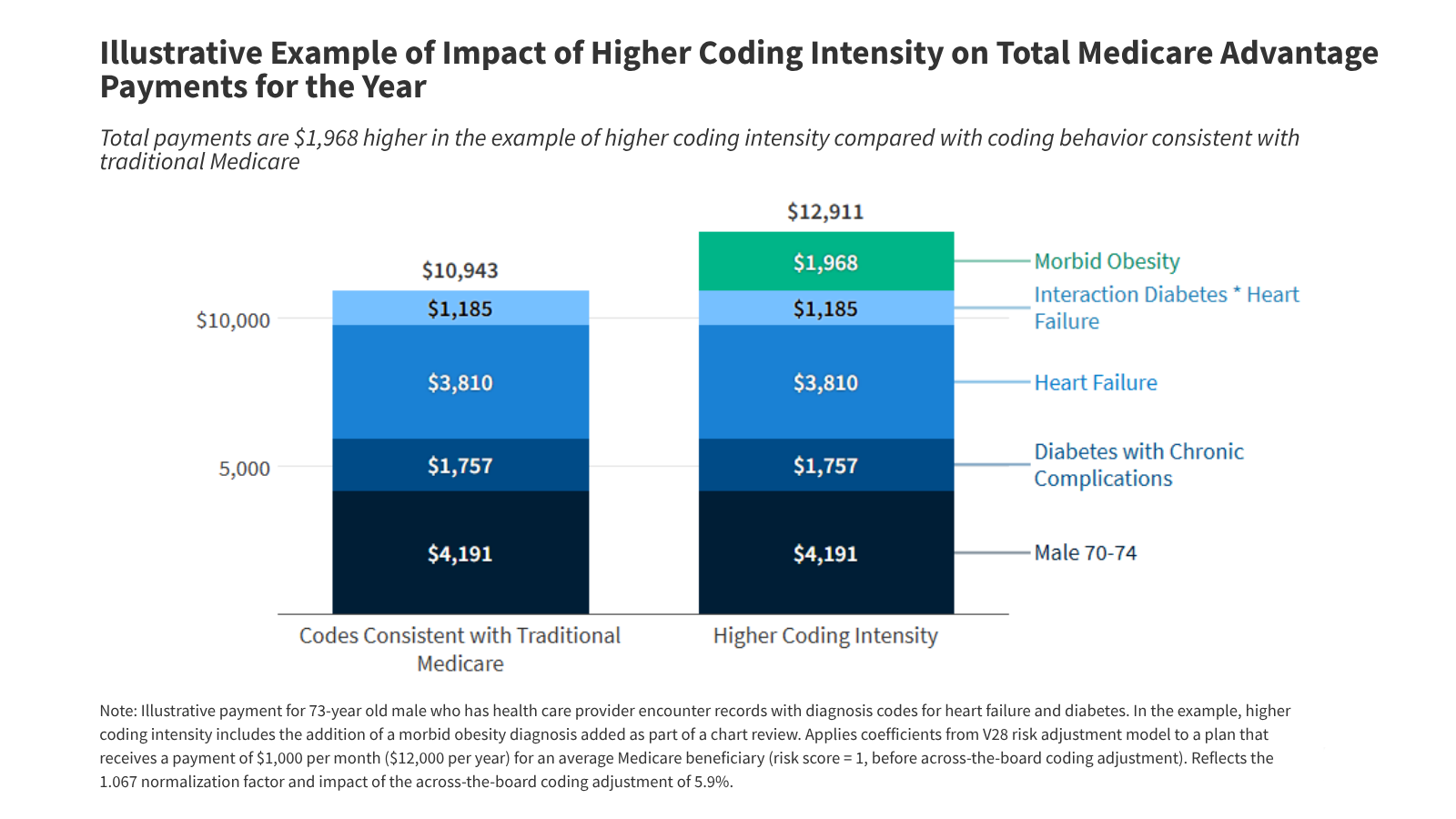
To visualize how this impacts the bottom line, consider a hypothetical 73-year-old enrollee, Mr. Smith, who suffers from type 2 diabetes and heart failure.
- Under Traditional Coding: His risk score reflects his known conditions. A standard calculation, after adjusting for normalization factors and mandated coding reductions, results in a plan payment of $10,943.
- Under Intensive Coding: If an insurer conducts a chart review and "discovers" a diagnosis like morbid obesity, Mr. Smith’s risk score climbs. The result? The plan receives $12,911—an 18% increase for a single added diagnosis code.
This practice is not isolated. KFF analysis reveals that chart reviews are the primary driver of coding intensity, often using AI-driven tools to scrub medical records for any mention of a condition that might trigger a higher payment bracket.
Official Responses and Industry Pushback
The reaction to these regulatory shifts has been bifurcated. CMS officials, led by the Biden-Harris administration, have consistently framed these changes as essential "accountability" measures. Their goal is to ensure that federal taxpayer dollars reflect actual patient care rather than administrative "upcoding."
Conversely, the insurance industry has been vocal in its opposition. Groups like the Better Medicare Alliance and AHIP have warned that the reduction in payments—specifically the exclusion of certain codes—will force plans to tighten their belts. Industry representatives argue that if federal payments are cut, the "extra" benefits that have become the hallmark of Medicare Advantage—such as dental, vision, hearing coverage, and reduced cost-sharing—will inevitably be on the chopping block.
However, data from the first two years of the V28 implementation suggests that the industry’s warnings may be overstated. While there have been modest increases in out-of-pocket limits and some trimming of supplemental benefits, insurers have absorbed the vast majority of the payment adjustments. Research indicates that insurers passed on only 17% to 24% of the payment reductions to the consumer, significantly less than the 50% "pass-through" seen in previous fiscal adjustments.
Implications for the Future of Medicare
The battle over coding intensity is far from over. Policymakers are now considering a variety of strategies to further bridge the gap between Medicare Advantage and traditional Medicare.
1. Expanding Exclusion Policies
There is significant support for broadening the list of diagnoses ineligible for risk adjustment. If "unlinked" chart reviews are disallowed, the next logical step, according to some advocates, is to exclude codes generated by health risk assessments (HRAs) that are not accompanied by a formal clinical encounter.
2. Tiered Adjustments
Rather than a flat, across-the-board reduction in risk scores, some economists have proposed a tiered system. Under this model, plans with historically high coding intensity would face larger downward adjustments to their risk scores, creating a more tailored approach to correcting for over-payment.
3. Addressing Favorable Selection
Perhaps the most significant, yet difficult, hurdle is "favorable selection." Even if coding intensity were perfectly mitigated, the fact remains that healthier people are more likely to join Medicare Advantage. This creates an inherent cost advantage that is not related to plan efficiency but to the demographics of the enrollee pool.
Proposals to fix this include:
- Benchmark Reform: Implementing a "discount rate" for MA benchmarks to account for the fact that MA enrollees, on average, have lower expected costs than those who stay in traditional Medicare.
- Clinical Data Integration: Using electronic health records (EHRs) and prescription drug claims to create a more robust risk profile that is applied equally to both traditional Medicare and MA.
- Two-Sided Reinsurance: A program where plans with significantly lower-than-average costs pay into a fund, which then supports plans that take on exceptionally high-cost, high-risk patients. This would neutralize the incentive to chase healthy enrollees.
Conclusion
The evolution of Medicare Advantage is at a crossroads. While the program has succeeded in providing broad, popular coverage to millions, the $76 billion gap in spending compared to traditional Medicare highlights a system in need of calibration. Coding intensity is the most visible manifestation of a payment model that rewards documentation over patient outcomes. As CMS continues to refine its risk adjustment models and tighten oversight, the challenge will be to ensure that the program remains fiscally sustainable without undermining the benefits that seniors have come to rely on. The coming years will be defined by whether the industry adapts to a more transparent, accuracy-focused payment environment, or if the friction between federal regulators and private insurers leads to further structural reform of the entire Medicare ecosystem.