As the Medicare Advantage (MA) program continues to serve as the primary delivery vehicle for private health insurance for millions of seniors, the "Quality Bonus Program"—an initiative born from the Affordable Care Act (ACA)—has come under intense scrutiny. Designed to incentivize high-quality care through a star-rating system, the program is now a multibillion-dollar fiscal pillar of the Medicare system. However, as spending reaches record highs, policymakers, regulators, and industry experts are questioning whether these bonuses are truly driving better health outcomes or simply inflating federal expenditures.
Main Facts: A Financial Snapshot
The Medicare Advantage quality bonus program rewards private health plans that achieve a star rating of 4 or higher on a five-star scale. These plans receive increased benchmark payments from the federal government, which they may—but are not required to—use to subsidize supplemental benefits like vision, dental, hearing aids, or reduced cost-sharing for enrollees.
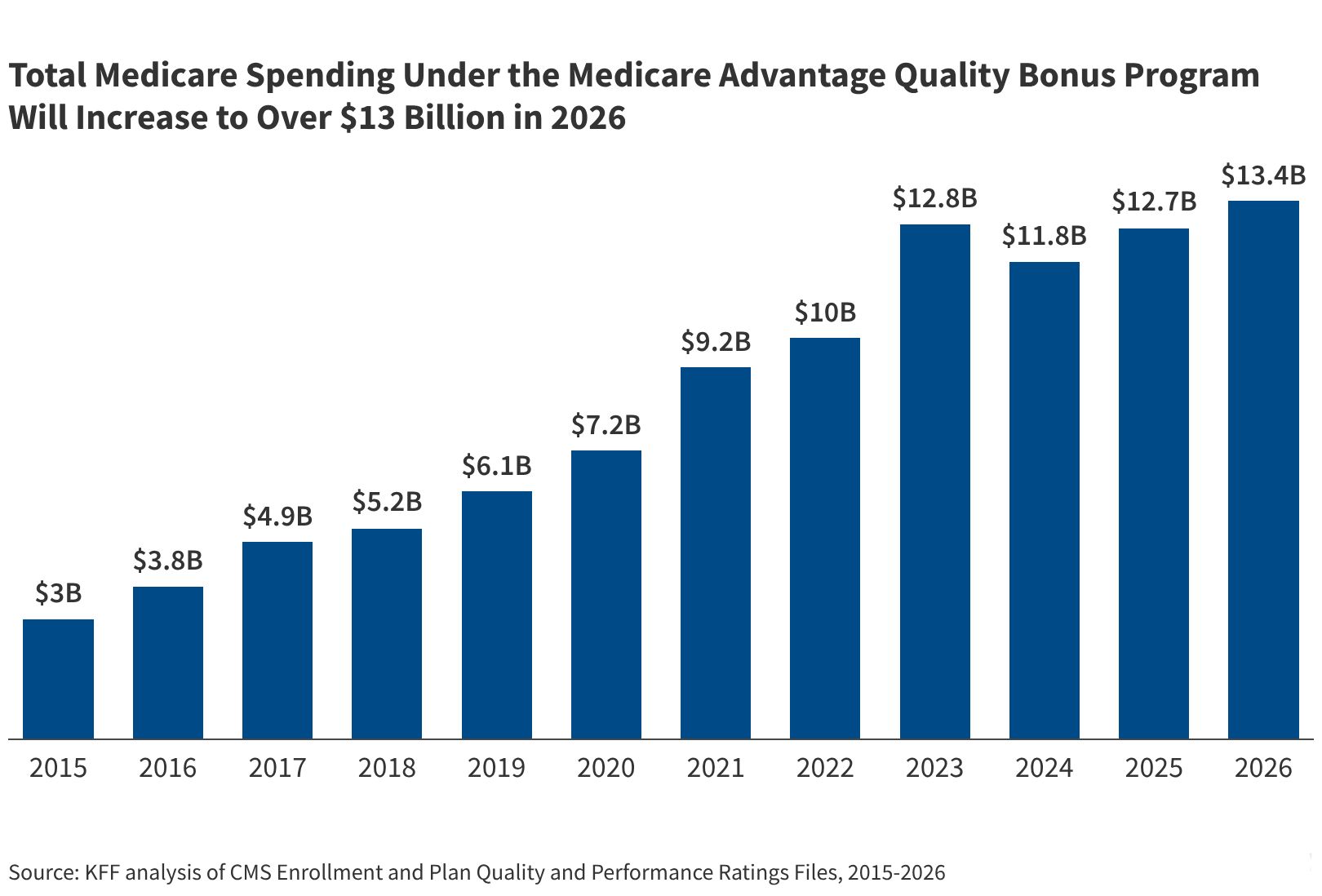
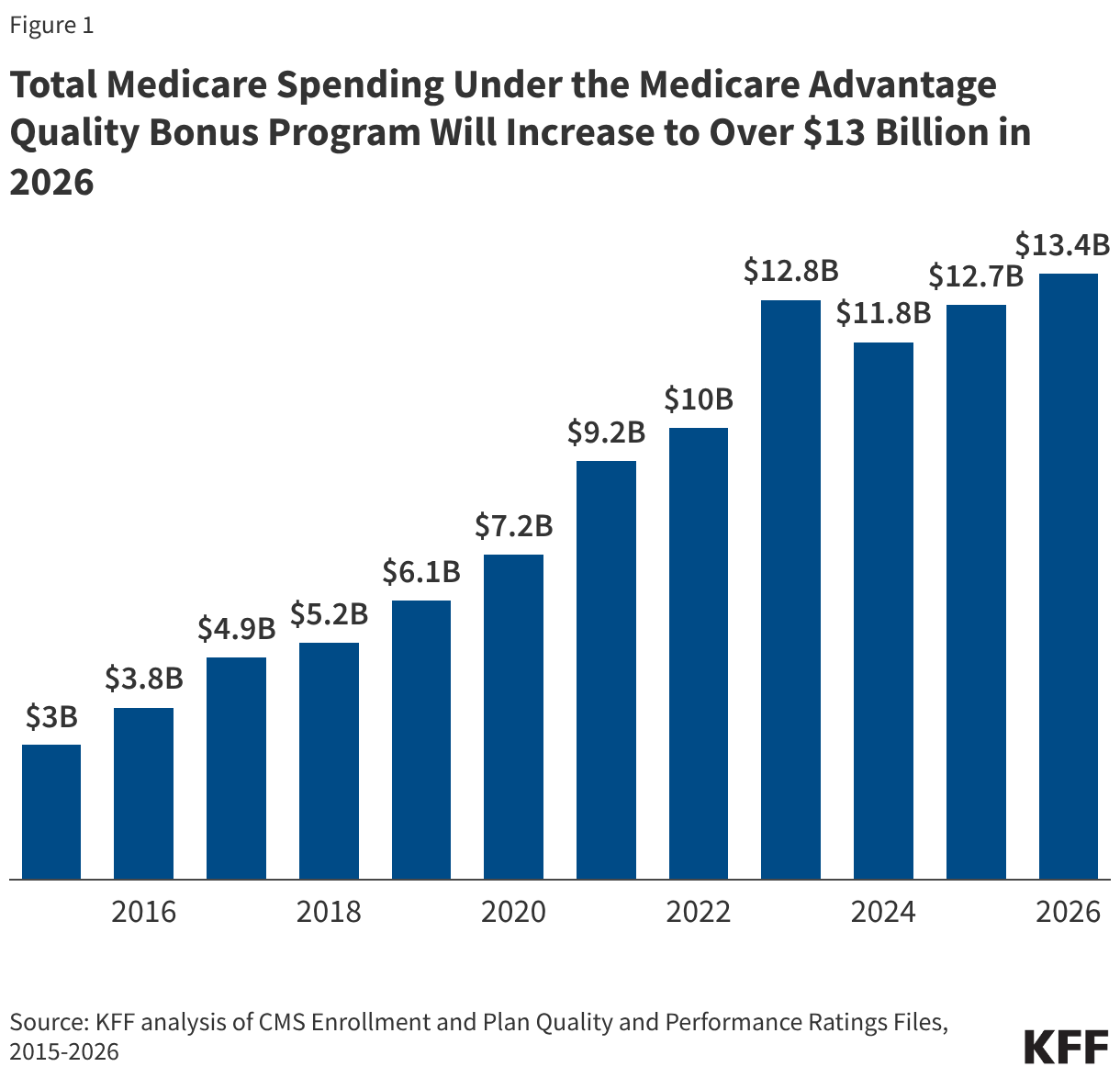
In 2026, federal spending on this bonus program is projected to hit at least $13.4 billion, a steady climb from $12.7 billion in 2025. This represents a staggering fourfold increase from the $3.0 billion spent in 2015. Today, these bonus payments account for 2.3% of the total projected $574 billion in Medicare Advantage payments.
Critics argue that these figures represent a lower bound. Because these estimates assume average health status for enrollees, they fail to account for the phenomenon of "coding intensity," where plans document higher levels of patient illness to increase risk-adjusted payments. The Medicare Payment Advisory Commission (MedPAC) estimates that once these risk-adjusted benchmarks are fully factored in, the actual impact of the bonus program on federal spending could be as high as $16 billion for 2026 alone.
Chronology: The Evolution of a Controversial Incentive
The program was established in 2010 as part of the Affordable Care Act, with the explicit goal of aligning private insurer behavior with clinical quality improvement.
- 2010–2015: The program was implemented, and the star rating system was standardized. During this period, enrollment in MA grew steadily, and the "bonus" mechanism became a standard feature of insurer revenue modeling.
- 2018: The Congressional Budget Office (CBO) issued a landmark analysis, projecting that eliminating the quality bonus program would save taxpayers nearly $100 billion over a decade. Since that report, MA enrollment has surged—reaching 35 million in 2026, 5 million more than the CBO’s initial projections—suggesting the potential savings from reform are now significantly higher.
- 2025–2026: A period of significant volatility. CMS introduced stricter cut-points for star ratings, leading to a decline in the number of contracts qualifying for bonuses. This caused financial friction for major carriers like Humana, which saw a notable dip in its star ratings, leading to public disputes and litigation between the industry and federal regulators.
- 2029 Projection: CMS has finalized changes to the star rating system, effective for the 2029 ratings, which will remove administrative measures that are no longer deemed effective at differentiating quality. While this simplifies the program, the transition is expected to increase federal spending by $18.6 billion over the next decade.
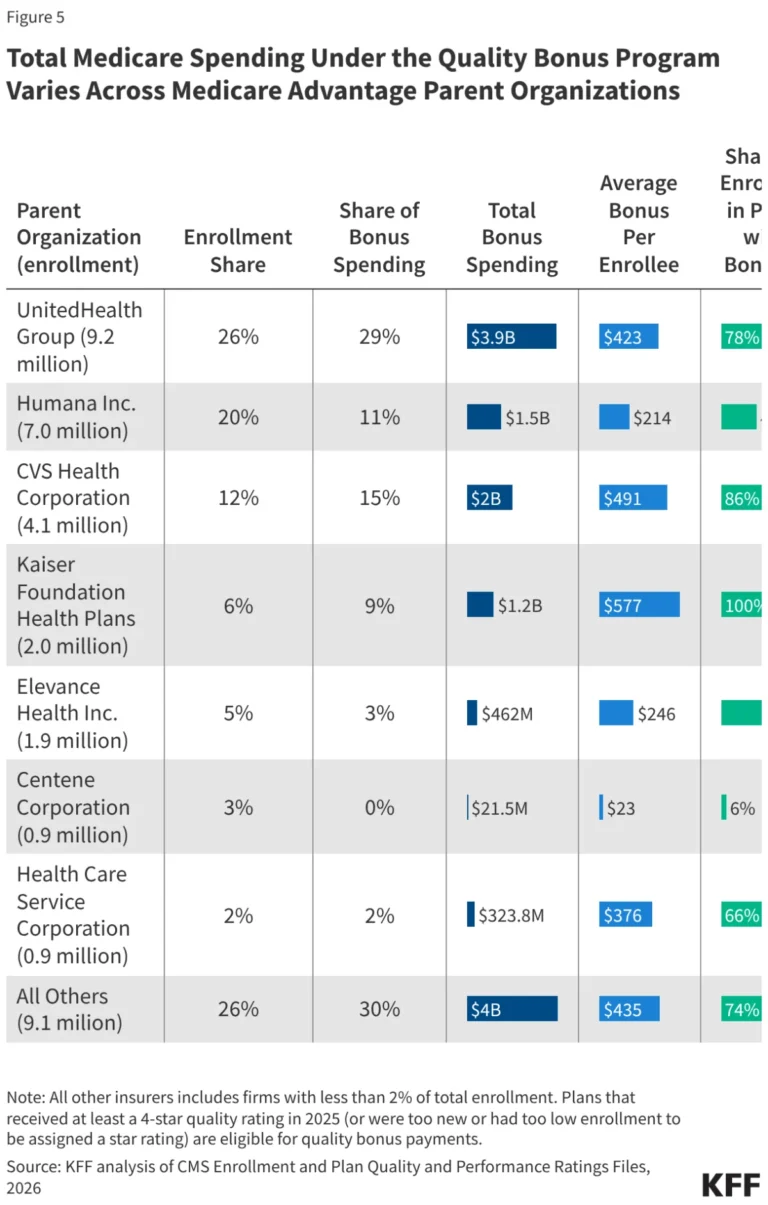
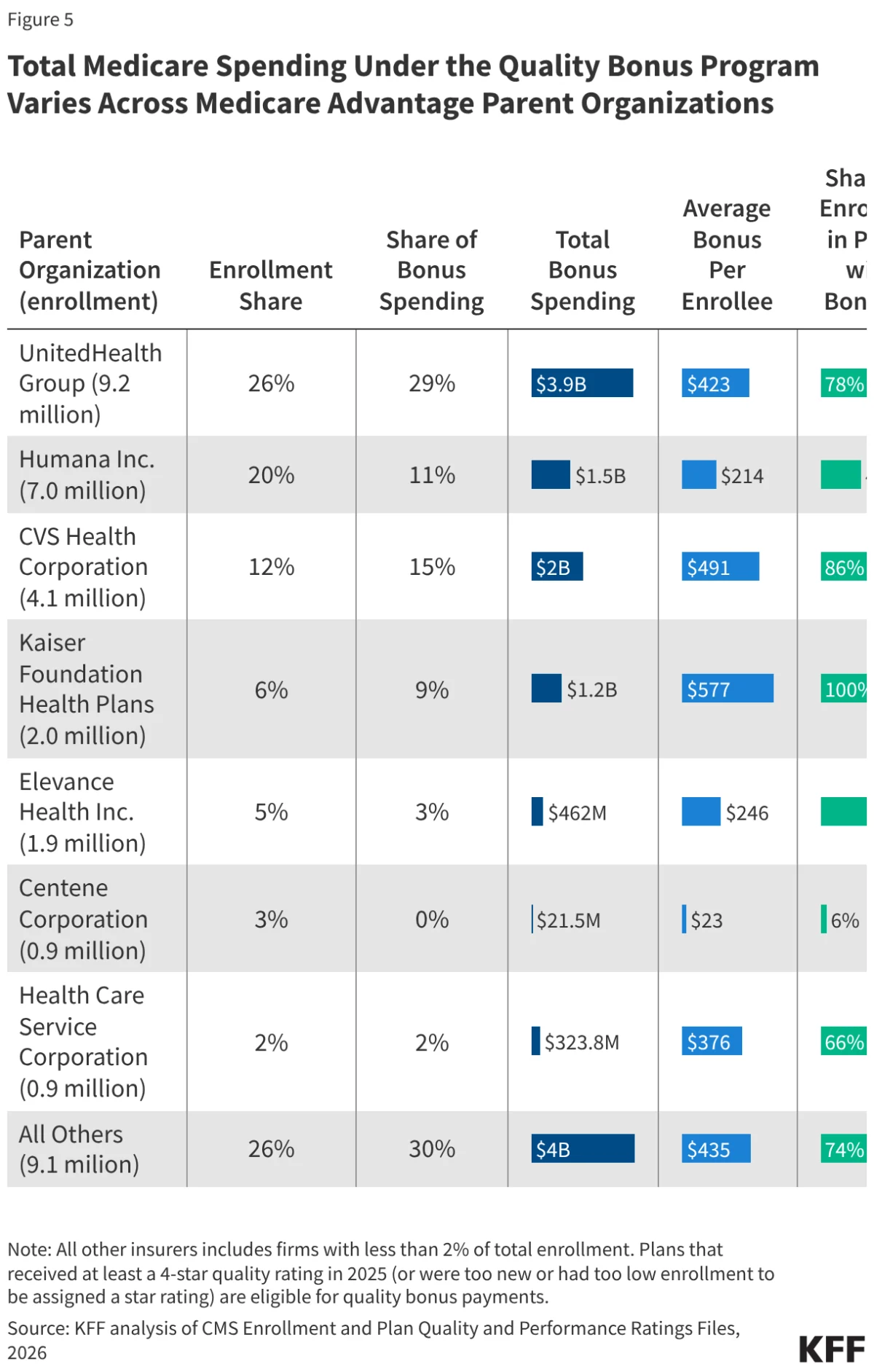
Supporting Data: The Disparity in Plan Performance
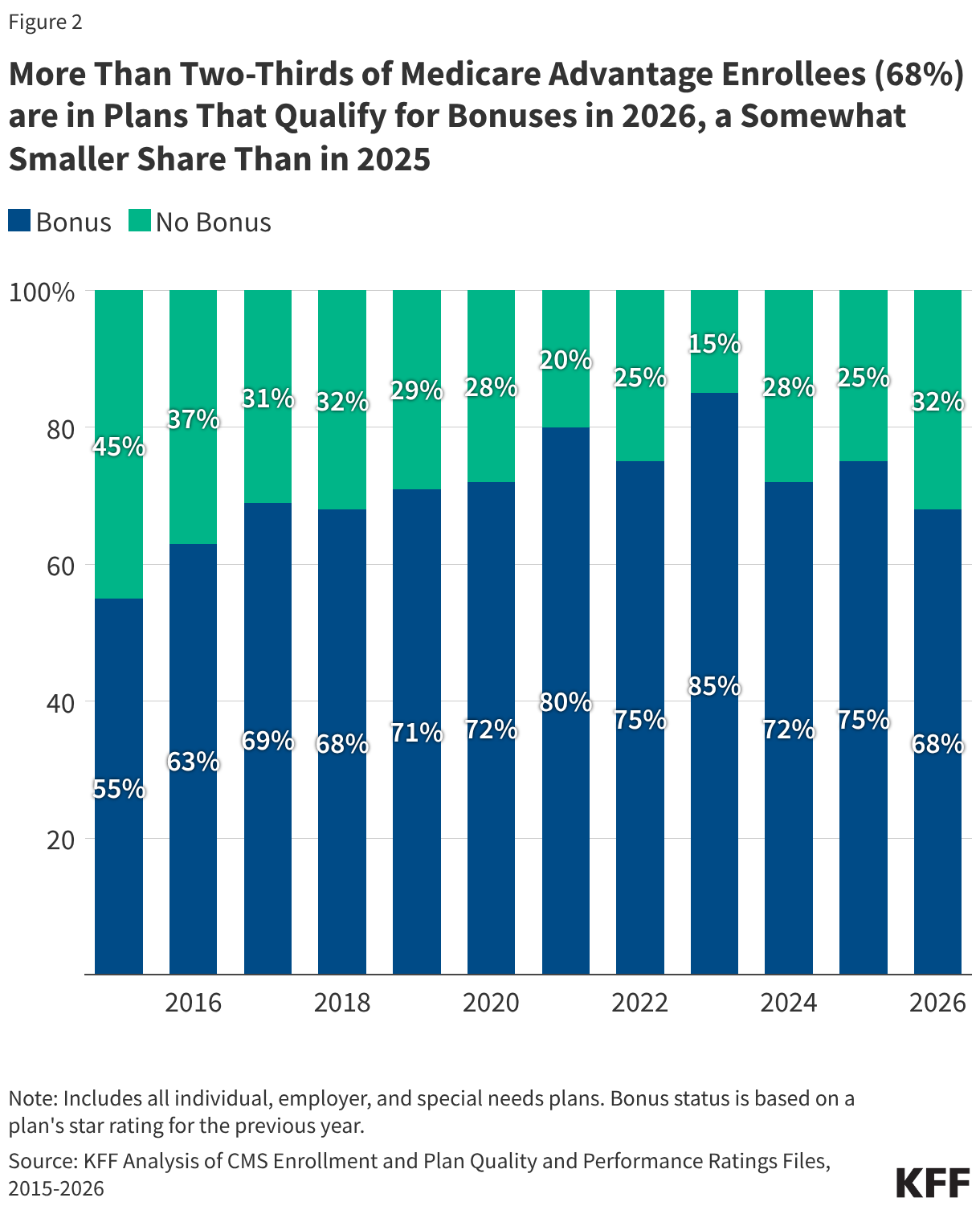
The program’s impact is not uniform across the insurance landscape. Currently, approximately 68% of all MA enrollees—nearly 24 million people—are in plans that qualify for quality bonuses. However, the distribution of these funds varies wildly by plan type and parent organization.
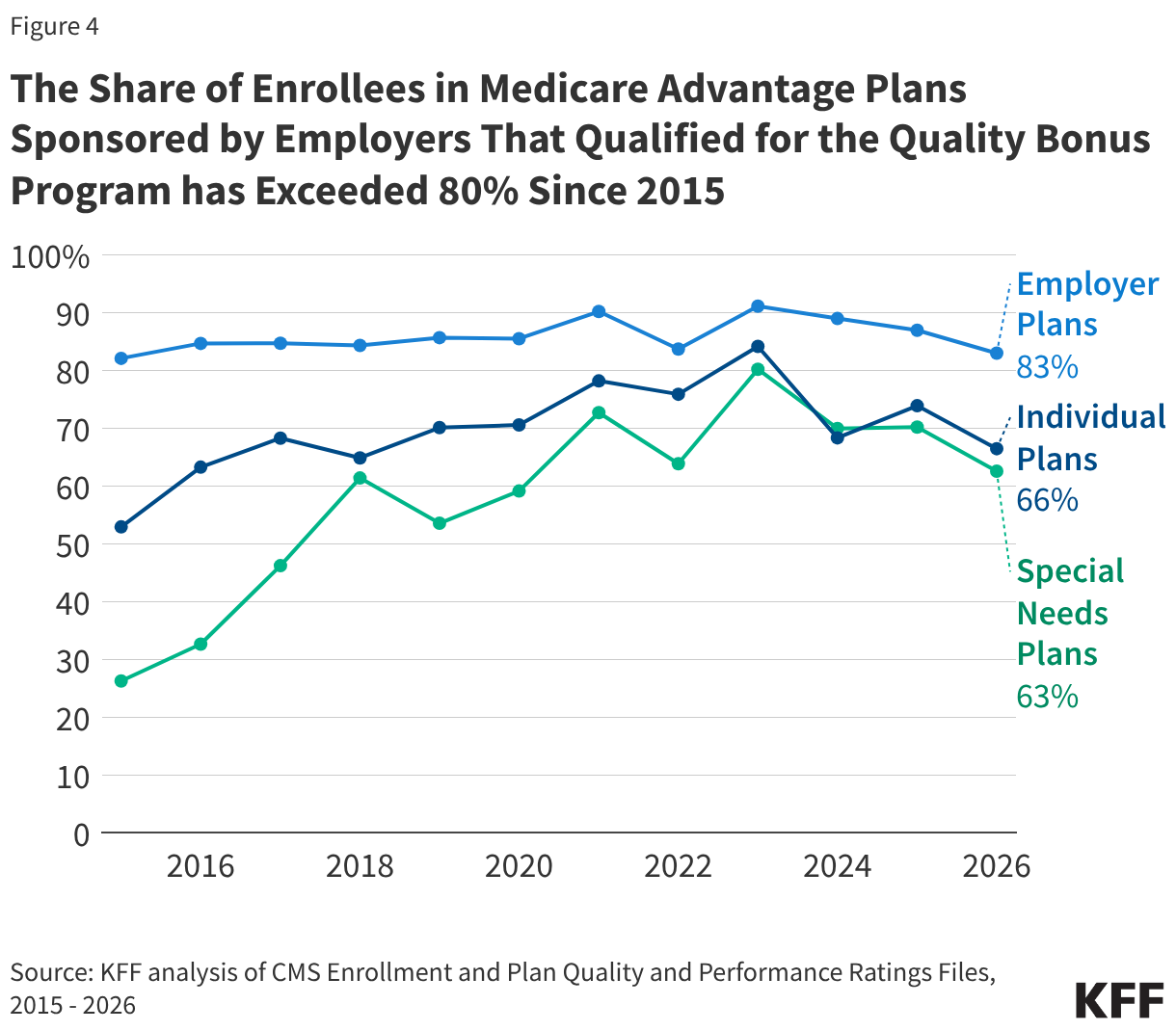
Employer-Sponsored Plans Lead the Way
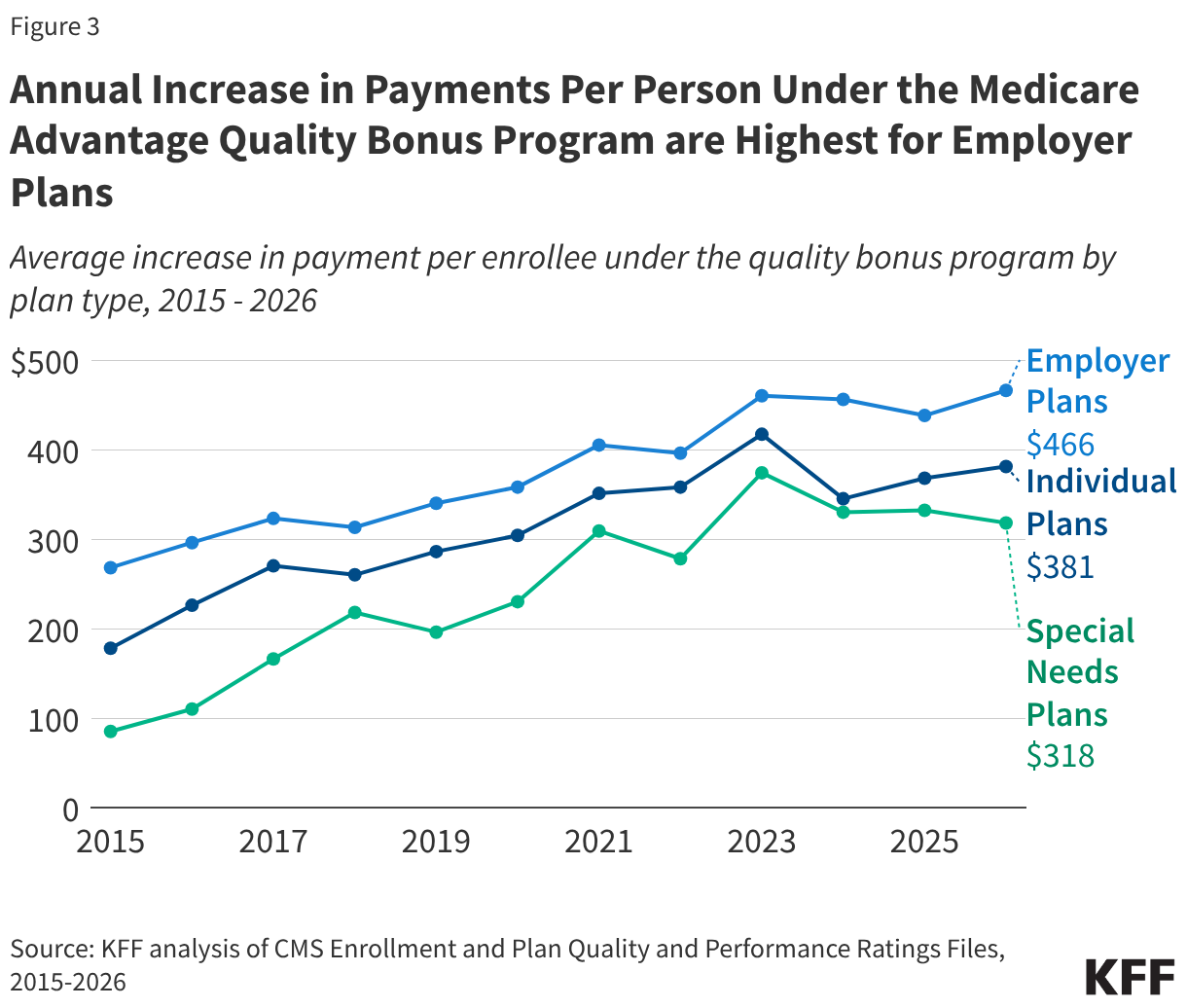
Employer- and union-sponsored Medicare Advantage plans consistently outperform individual and special needs plans (SNPs) in achieving high star ratings. Data indicates that over 80% of enrollees in employer-sponsored plans have been in bonus-eligible plans every year since 2015. Consequently, the average annual payment increase per enrollee for these plans is $466, significantly higher than the $381 for individual plans and the $318 for SNPs.
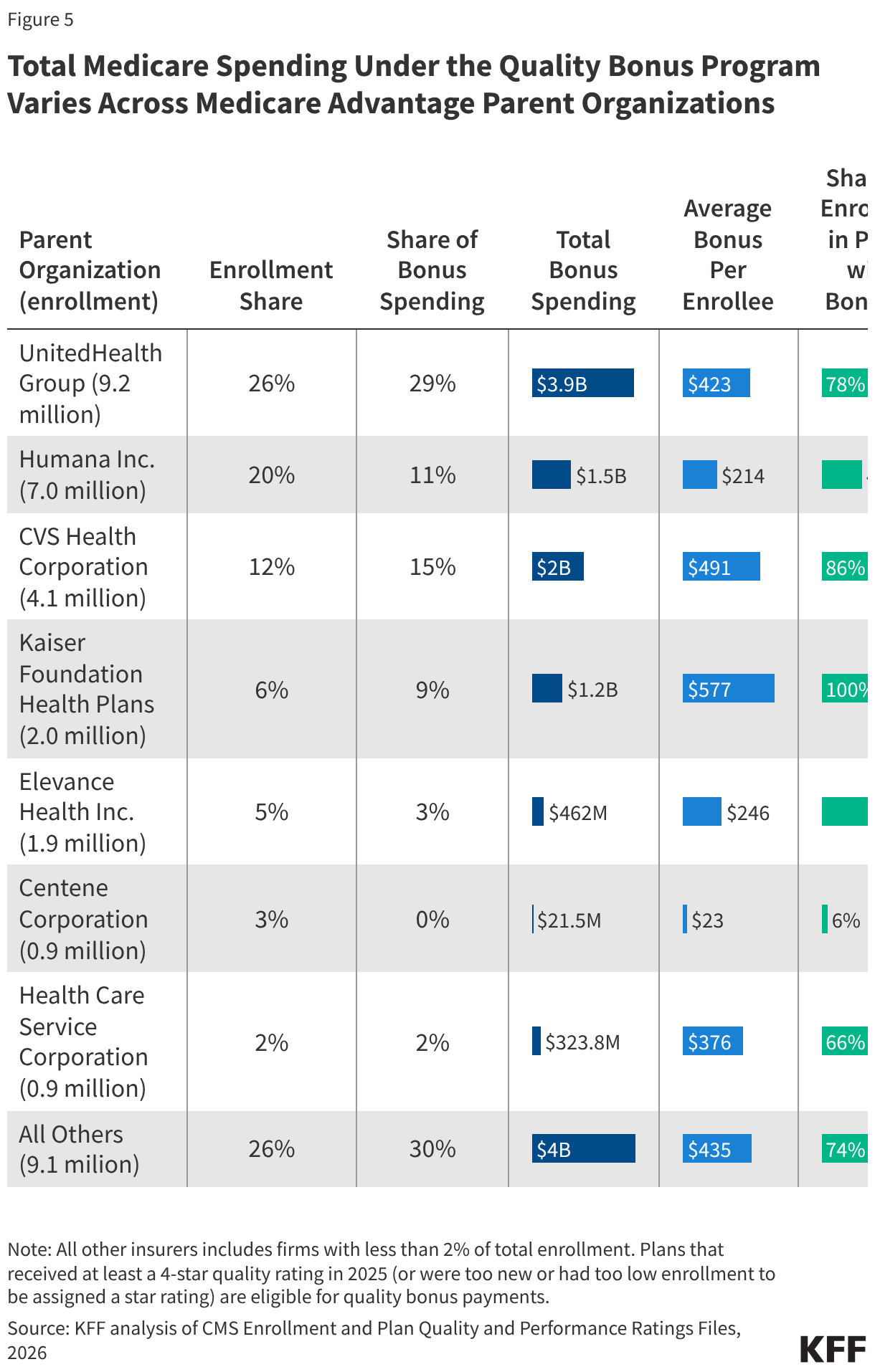
The "Corporate" Divide
The financial benefit of the program is heavily concentrated among the largest insurers. UnitedHealth Group, which commands 26% of the MA market, is expected to capture 29% of the total bonus spending in 2026—roughly $3.9 billion. In contrast, Humana’s share of the bonus pool has contracted following recent rating adjustments.
Perhaps most illustrative of the system’s inconsistency is the variance between firms: Kaiser Foundation Health Plans sees 100% of its 2 million enrollees in bonus-eligible plans, while only 6% of Centene’s 938,000 enrollees are in such plans. This suggests that the "quality" bonus is as much a reflection of organizational administrative capability as it is of clinical excellence.
Official Responses and Regulatory Challenges
The Centers for Medicare & Medicaid Services (CMS) maintains that the star rating system is a vital tool for consumer choice. By publishing these ratings, CMS intends to help beneficiaries navigate a complex marketplace. However, the system has faced fierce criticism from independent watchdogs.
MedPAC has repeatedly argued that the star ratings incorporate too many measures, many of which do not meaningfully distinguish high-performing plans from average ones. Furthermore, because ratings are reported at the "contract" level rather than the "plan" level, a single contract may cover multiple plans with vast differences in networks and benefits. This masks poor performance in specific, vulnerable segments of the population.
Insurers have responded to these regulatory pressures with increasing litigiousness. When CMS recalculates cut-points or removes measures, carriers have increasingly turned to the courts, arguing that the methodology is arbitrary. While some insurers have won limited concessions—such as the recent recalculation of 2026 star ratings following a challenge from Clover Health—these legal battles underscore a fundamental lack of consensus on what "quality" actually means in the context of Medicare Advantage.
Implications: A System in Need of Reform?
The long-term sustainability of the Medicare Advantage quality bonus program is now a central debate in federal health policy. The implications of the current trajectory are threefold:
- Fiscal Pressure: As Medicare faces long-term solvency challenges, the rapid growth of bonus payments is being scrutinized as a contributor to the widening spending gap between private MA plans and traditional fee-for-service Medicare.
- Equity Concerns: The fact that employer-sponsored plans—which often cover healthier, more affluent retirees—consistently receive higher bonus payments than Special Needs Plans (which serve the dual-eligible and chronically ill) raises serious questions about the program’s ability to promote equity. If the goal of the program is to improve health outcomes, current data suggests it may be inadvertently rewarding plans with the easiest-to-serve populations.
- The "Quality" Myth: If the star ratings do not effectively differentiate quality, then the multibillion-dollar transfer of funds is essentially a subsidy rather than a performance-based incentive. Without a significant overhaul of how quality is measured—or a move toward different payment structures—the program risks becoming a permanent, inefficient fixture of the federal budget.
As Congress debates the future of Medicare, the Quality Bonus Program stands at a crossroads. Lawmakers must decide whether to continue refining the current star-rating methodology, or to consider more radical alternatives—such as capping bonus payments or shifting toward a value-based model that prioritizes outcomes for the most vulnerable enrollees over the administrative metrics of the largest carriers. Until such reforms are implemented, the program will likely remain a flashpoint for both fiscal conservatives and health policy advocates who argue that Medicare should be paying for care, not just for the status of a plan’s administrative rating.