The intersection of a life-threatening medical diagnosis and a family’s most joyous milestones creates a unique emotional landscape. For Alice Tawil, 2025 was a year defined by this very duality: the frightening uncertainty of a Stage 1 Triple Negative Breast Cancer (TNBC) diagnosis and the celebratory preparations for her son’s wedding. Her journey, marked by aggressive treatment and the vital support of specialized advocacy groups, serves as a poignant case study in the importance of early detection, personalized oncology, and the power of community-based psychosocial support.
Main Facts: The Diagnosis and Clinical Response
In February 2025, Alice Tawil underwent what was intended to be a routine mammogram. Like many women her age, the screening was a standard preventative measure, not prompted by any specific symptoms or palpable lumps. However, the imaging revealed a suspicious mass, leading to a swift biopsy that confirmed the presence of a tumor.
While many breast cancers are driven by hormones—estrogen or progesterone—or the HER2 protein, Tawil’s pathology report indicated a more challenging subtype: Triple Negative Breast Cancer (TNBC). TNBC is characterized by the absence of these three common receptors, meaning it does not respond to hormonal therapy or drugs that target HER2.
Initially, the clinical expectation was that a lumpectomy followed by minor medication and localized radiation would suffice. However, the aggressive nature of TNBC necessitated a more rigorous intervention. Tawil’s medical team at the oncology center pivoted the care plan to include systemic chemotherapy to ensure any microscopic cancer cells were eradicated, followed by a concentrated course of radiation.
The cornerstone of Tawil’s recovery was not just medical, but also logistical and emotional. Upon the recommendation of a friend, she connected with Sharsheret, a national non-profit organization dedicated to supporting Jewish women and families facing breast and ovarian cancer. This partnership proved instrumental in navigating the complexities of her treatment.
Chronology of a Crisis: From Screening to the Altar
The timeline of Alice Tawil’s experience illustrates the rapid pace at which modern oncology must move when dealing with aggressive pathologies.
February 2025: The Discovery
The journey began with the routine mammogram. Within days, the diagnostic process escalated from imaging to a biopsy, and finally to a surgical consultation. The initial diagnosis of a "small tumor" provided a brief, albeit false, sense of security that the treatment would be minimally invasive.
Spring 2025: The Shift in Strategy
Following the lumpectomy and a deeper analysis of the tumor’s pathology, the diagnosis was refined to Stage 1 Triple Negative Breast Cancer. It was at this juncture that the oncologist recommended four rounds of chemotherapy. This period coincided with the engagement of Tawil’s son. Balancing the physical toll of chemotherapy with the social demands of hosting an engagement party became a defining challenge. At this stage, Tawil chose to keep her diagnosis private, sharing the news only with her immediate family to keep the focus on her son’s happiness.
Summer 2025: The Treatment Arc
As the chemotherapy sessions began, the physical manifestations of the disease—most notably hair loss—became a reality. It was during this time that Sharsheret’s involvement intensified. Tawil was assigned a dedicated social worker who provided a consistent point of contact for emotional support and practical resources. The four rounds of chemotherapy were followed by 15 sessions of radiation, a grueling schedule designed to minimize the risk of recurrence.
September 2025: Recovery and Celebration
The culmination of Tawil’s medical journey was timed almost poetically with her family’s personal milestone. She completed her final radiation session just one week before her son’s wedding. The ability to attend the ceremony not as a patient in active treatment, but as a survivor in recovery, marked the end of an intense seven-month ordeal.
Supporting Data: Understanding Triple Negative Breast Cancer
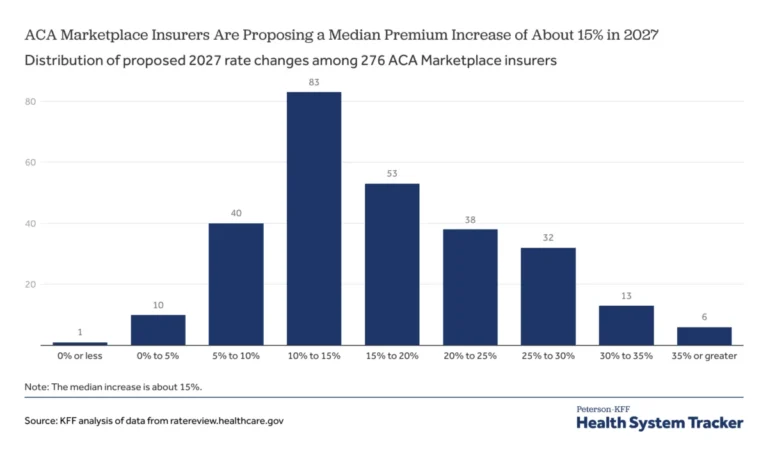
To understand the gravity of Tawil’s journey, one must examine the clinical profile of Triple Negative Breast Cancer. TNBC accounts for approximately 10% to 15% of all breast cancer cases. It is widely considered more aggressive than other subtypes because it grows faster, is more likely to have spread by the time it is found, and has a higher likelihood of recurrence after treatment.
The Biological Challenge
In most breast cancers, oncologists use "targeted" therapies. For example, if a cancer is estrogen-receptor-positive, drugs like Tamoxifen can be used to block the hormones that fuel the cancer. Because TNBC lacks these receptors, these targeted "silver bullets" are ineffective. Consequently, chemotherapy remains the primary systemic treatment.

Prevalence and Demographics
While TNBC can affect anyone, research indicates it is more prevalent among:
- Women under the age of 40.
- Black and Hispanic women.
- Individuals with a BRCA1 genetic mutation.
Given the higher prevalence of BRCA mutations within the Ashkenazi Jewish population, organizations like Sharsheret play a critical role in providing culturally competent care and genetic screening resources.
The Importance of Staging
Tawil’s diagnosis at "Stage 1" was a critical factor in her positive outcome. At Stage 1, the cancer is localized and hasn’t spread to the lymph nodes. For TNBC, early detection is particularly vital because of how quickly the cells divide. A delay of even a few months could have resulted in a higher stage diagnosis, requiring significantly more invasive treatment and a lower statistical probability of long-term remission.
Official Responses: The Role of Sharsheret and Psychosocial Care
The medical community increasingly recognizes that treating the tumor is only one half of the battle; treating the patient’s mental and emotional well-being is the other. Alice Tawil’s reliance on Sharsheret highlights a growing trend in "whole-patient" oncology.
The Social Work Connection
Sharsheret’s model involves pairing patients with specialized social workers. In Tawil’s case, this professional provided more than just clinical information; she provided "warmth and encouragement" during the traumatic experience of hair loss. This form of psychosocial intervention is proven to reduce cortisol levels and improve treatment adherence in cancer patients.
Practical Support Kits
The organization also utilizes "care packages" as a tool for empowerment. Tawil received:
- Educational Resources: Clarifying the specifics of TNBC to reduce the "fear of the unknown."
- Healthy Cookbooks: Addressing the nutritional needs of patients undergoing chemotherapy.
- Exercise Bands: Encouraging physical activity, which is linked to reduced fatigue during radiation.
- Comfort Items: A soft blanket and pillow, which Tawil noted she brought to every session, providing a sense of "home" in a sterile clinical environment.
By addressing the practicalities of the patient experience, support organizations bridge the gap between the hospital and the home.
Implications: Lessons for the Public and the Medical Community
Alice Tawil’s story offers several broader implications for public health and the future of oncology.
The Efficacy of Routine Screening
Tawil’s experience is a resounding endorsement for routine mammography. Had she waited until a lump was palpable, her TNBC might have progressed beyond Stage 1. Her story serves as a reminder that "feeling well" is not a substitute for clinical screening.
The Burden of the "Silent Patient"
Tawil’s decision to keep her diagnosis private during her son’s engagement highlights the emotional burden patients often carry to protect their loved ones’ joy. This "double life"—being a joyful mother of the groom by day and a chemotherapy patient by night—requires immense psychological resilience. It also underscores the need for private support networks where patients can be honest about their struggles without fear of "ruining" a family occasion.
The Future of TNBC Research
While Tawil’s treatment consisted of traditional chemotherapy and radiation, the landscape for TNBC is shifting. New developments in immunotherapy, such as the use of pembrolizumab (Keytruda), are beginning to offer new hope for TNBC patients, particularly those with higher-stage diagnoses. Tawil’s success with the current standard of care provides a benchmark for these emerging therapies.
Conclusion
Alice Tawil’s journey from a February mammogram to a September wedding is a testament to the advancements in modern oncology and the necessity of robust support systems. By combining aggressive medical intervention with the compassionate guidance of Sharsheret, she was able to navigate the "triple negative" storm and emerge in time to celebrate a new chapter in her family’s life. Her story encourages others facing similar diagnoses to seek out specialized support, reminding them that while the diagnosis is a part of their life, it does not have to be the end of their joy.